{kind=link}
{kind=link}
{kind=link}
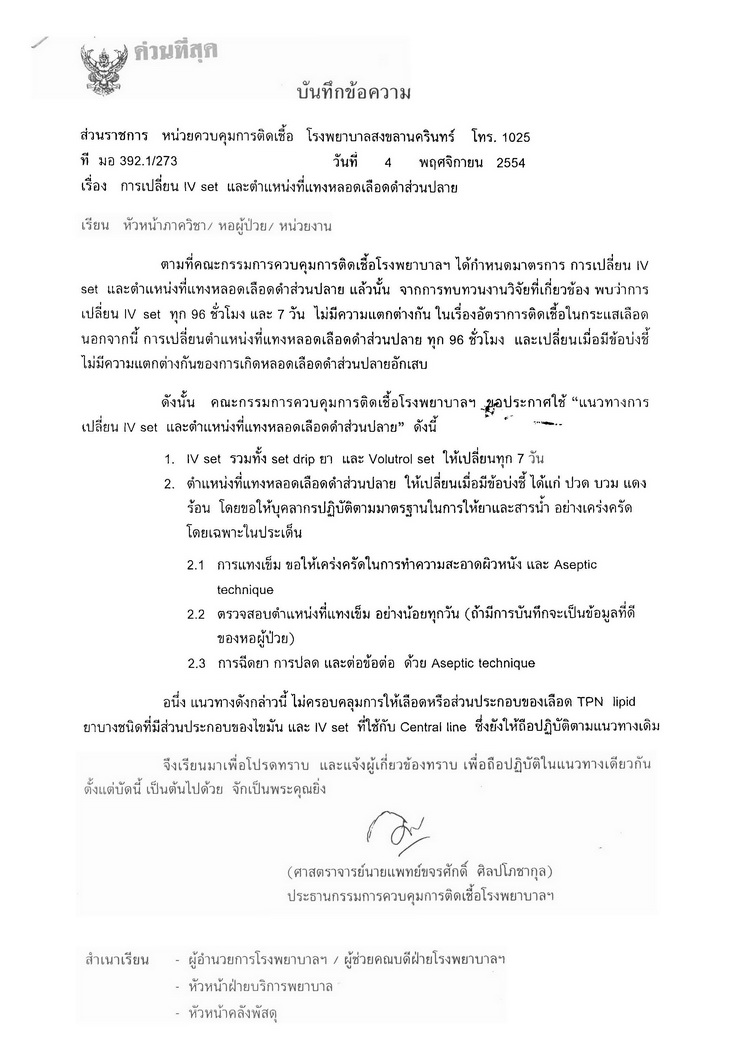 คณะกรรมการควบคุมการติดเชื้อ รพ. ได้ทบทวนข้อมูลและเวียนแจ้งในบันทึกข้อความ ที่แนบแล้วค่ะ Posted by : icn , Date : 2012-07-18 , Time : 11:11:15 , From IP : 172.29.10.197 |
ลองอ่านดูนะคะว่าตกลง Current Evidence recommended ให้เปลี่ยนตำแหน่ง IV ทุกกี่วัน; Controversial issue regarding optimal durationถึงพี่ ๆ น้อง ๆ พยาบาล มอ โดยเฉพาะท่านที่ร่วม Discuss เกี่ยวกับ Evidenceเรื่อง ระยะเวลาที่เหมาะสมในการเปลี่ยนตำแหน่งให้ IV ลองดู Paper ปี 2011 ทั้งของ BSI และของ Professor Claire Rickard ลอง key search ตาม Title ด้านล่างนี้นะคะ (พอดี link file ไม่เป็น) Routine resite of peripheral intravenous devices every 3 days did not reduce complications compared with clinically indicated resite: a randomised controlled trial Claire M Rickard1*, Damhnat McCann2, Jane Munnings3, Matthew R McGrail4 * Correspondence: c.rickard@griffith.edu.au 1Research Centre for Clinical and Community Practice Innovation, Griffith University, 170 Kessels Rd, Nathan Qld 4111, Australia Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011 Systematic Review of Infection Control Literature Relating to Intravascular Devices Professor Claire Rickard & Ms Gillian Ray-Barruel Griffith University ระวัง! อย่าลืมหาอะไรเกาะไว้ให้แน่นขณะอ่าน มิฉะนั้นจะตก Trend เหมือนดิฉันค่ะ แงๆๆๆๆๆๆๆๆๆๆๆๆๆๆๆๆๆๆๆ Enjoy Reading B Posted by : khomapak , E-mail : (khomapak.m@psu.ac.th) , Date : 2012-07-18 , Time : 01:35:52 , From IP : 115.67.192.7 |
|
มาช่วยใส่ลิงค์ให้ไปถึงง่ายๆค่ะ " Routine resite of peripheral intravenous devices every 3 days did not reduce complications compared with clinically indicated resite: a randomised controlled trial น่าสนใจนะคะ คุณแม่พี่แกจะให้ถอดออกเมื่อไหร่ที่แกรู้สึกเจ็บค่ะ บางทีก็ต้องขึ้นกับบริบทของคนไข้แต่ละคนด้วยใช่ไหมคะ Posted by : anothai , Date : 2012-07-18 , Time : 03:31:42 , From IP : 172.29.5.236 |
|
อันนี้ดีจังค่ะ ของ CDC ได้มาทั้งเอกสารเลย " Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011 Posted by : anothai , Date : 2012-07-18 , Time : 03:36:21 , From IP : 172.29.5.236 |
|
คณะกรรมการควบคุมการติดเชื้อ รพ. ได้ทบทวนข้อมูลและเวียนแจ้งในบันทึกข้อความ ที่แนบแล้วค่ะ Posted by : icn , Date : 2012-07-18 , Time : 11:11:15 , From IP : 172.29.10.197 |
|
ขอบพระคุณหน่วย ICN มาก ๆ ค่ะและจะขออนุญาต circulate ให้กับทางคณะพยาบาลฯ คือ จริง ๆ เวลาพา นศ ไป เราก็พยาม Strict ตาม latest current update ของ รพ และเชื่อมั่นว่าการเปลี่ยนแปลงต้องมี Best evidence supported แน่นอนค่ะ เพียงแต่ยังไม่ได้มีเวลาหา Evidence paper มา share กัน และเนื่องจากพวกเราต้อง academic shopping ไปถึง 3 รพ จึงเกิด controversial in the same issue ซึ่ง re-site IV ก็เป็นหนึ่งในเรื่องที่ต่างกันทั้ง 3 รพ ค่ะ เมื่อวานที่เราสัมมากันทั้งอาจารย์ในคณะและตัวแทนพี่ ๆ จากทั้ง 3 รพ เราก็จะจับมือมา June กันโดยใช้ High grade level of the latest current evidence ของแต่ละเรื่องเป็นหลัก ของเมื่อวานเรามีแต่ paper 2004 (ซึ่ง out-of-date) พอเจอ 2011 ซึ่ง สอดคล้องกับที่ทาง รพ ทำอยู่แล้ว นอกจากนี้ยังมีในเรื่องของการ Dressing และ Indwelling urinary catheter ประเด็นหลักจริง ๆ คือ เรากำลังจะ Reengineering การสอน Fundamental nursing ของเราโดยใช้ EBP ค่ะ และที่ฝันสุด ๆ คือ ภายหลังจากที่เราปรับแล้วหน่วยที่เป็นแหล่งฝึกอู่ข้าวอู่น้ำของเราทั้ง 3 แหล่งจะใช้หลักการเดียวกัน ขอรบกวนสอบถามเพิ่มเติมในเรื่องของการตรวจสอบตำแหน่งที่แทงเข็มซึ่งส่วนตัวเข้าใจว่าเป็นการประเมิน Phlebitis and occlusion ในมุมมองของพยาบาลตรงนี้รู้สึกเป็นห่วงว่าพยาบาลทุกคนจะเข้าใจชัดเจนตรงกันเป็นรูปธรรม หรือใช้เกณฑ์เดียวกันในการประเมินหรือไม่ ซึ่งตรงนี้หากได้ inform เกณฑ์ที่ชัดเจนแล้วก็คงไม่น่าเป็นห่วงค่ะ ถ้ายังไงรบกวนช่วย forward ให้ด้วยนะคะจะได้แจกจ่ายต่อในคณะฯ สำหรับตัวเองตอนนี้ ใช้ตามหลักที่ Review เองของปี 2011 ที่ว่า "Phlebitis was defined as a total score of 2 or more points from the following factors: pain (on a 10-point scale, 1 p 1 point, and 2 or more p 2 points); redness (less than 1 cm p 1 point, and 1 or more cm p 2 points);swelling (as for redness); and discharge (hemoserous ooze under dressing p 1 point, and hemoserous ooze requiring dressing change or purulence p 2 points)." และ Occlusion was defined as the inability to inject or aspirate. Compared withother definitions that usually require at least 2 symptoms (eg, pain and redness), สุดท้ายนี้ขอบคุณอีกครั้งนะคะทั้งพี่แต๋ว หน หน่วย และ staff ทุก ๆ ท่าน และไหน ๆ แล้วขอรบกวนอีกเรื่องว่าหากมีการ update มฐ อีกเมื่อไหร่ รบกวนช่วย forward ข้ามฟากมาให้ด้วยนะคะ เพราะบางครั้งก็ไม่ได้ review บ่อย ๆ จริง ๆ ค่ะ Posted by : khomapak , E-mail : (khomapak.m@psu.ac.th) , Date : 2012-07-18 , Time : 13:04:17 , From IP : 192.168.29.184 |
|
เมื่อกล่าวถึง phlebitis อาจะต้องมองใน 2 ด้าน ว่าสิ่งที่เราประเมินได้ เป็น phlebitis หรือ inflammation และ สาเหตุมาจาก mechanical,chemical หรือว่าเป็นจาก infectious เป็นที่ทราบกันดีว่า risk ของ peripheral line ต่อ infection ค่อนข้างน้อย แต่การเฝ้าระวังเป็นการเพิ่มคุณภาพการพยาบาล การดำเนินการต้องครอบคลุมทั้งการป้องกันการติดเชื้อและการประเมิน early sign เนื่องจากในกรณีที่ให้สารละลายที่มีความเข้มข้นสูง ถึงแม้เราจะ care exit site อย่างดี ล้างมือตามข้อบ่งชี้ ปฏิบัติตาม aseptic technique แต่ phlebitis ก็ยังเกิดได้ ดังนั้นการประเมินตำแหน่งที่แทงจึงมีความสำคัญเช่นกัน การ monitor ใช่เพียงจะบอกว่าเกิดหรือไม่เกิด Phlebitis แต่การ detect ได้เร็วจะเป็นสิ่งที่ดีที่สุด สำหรับการประเมิน phlebitis นิยมใช้เกณฑ์ ดังนี้ phlebitis scale Grade 0 No symptoms Grade 1 Erythema at access site with or without pain Grade 2 Pain at access site with erythema and/or oedema Grade 3 Pain at access site with erythema and/or oedema, streak formation, palpable venous cord Grade 4 Pain at access site with erythema and/or oedema, streak formation, palpable venous cord greater than one inch in length and purulent drainage Source: Infusion Nurses Society (2006) Posted by : pranee , E-mail : (apranee@medicine.psu.ac.th) , Date : 2012-07-18 , Time : 21:03:51 , From IP : 113.53.30.137 |
| ความเห็นจาก Social Network : Facebook |
|
|
>>>>> Page loaded: 0.006 seconds. <<<<< |
{kind=link}
{kind=link}