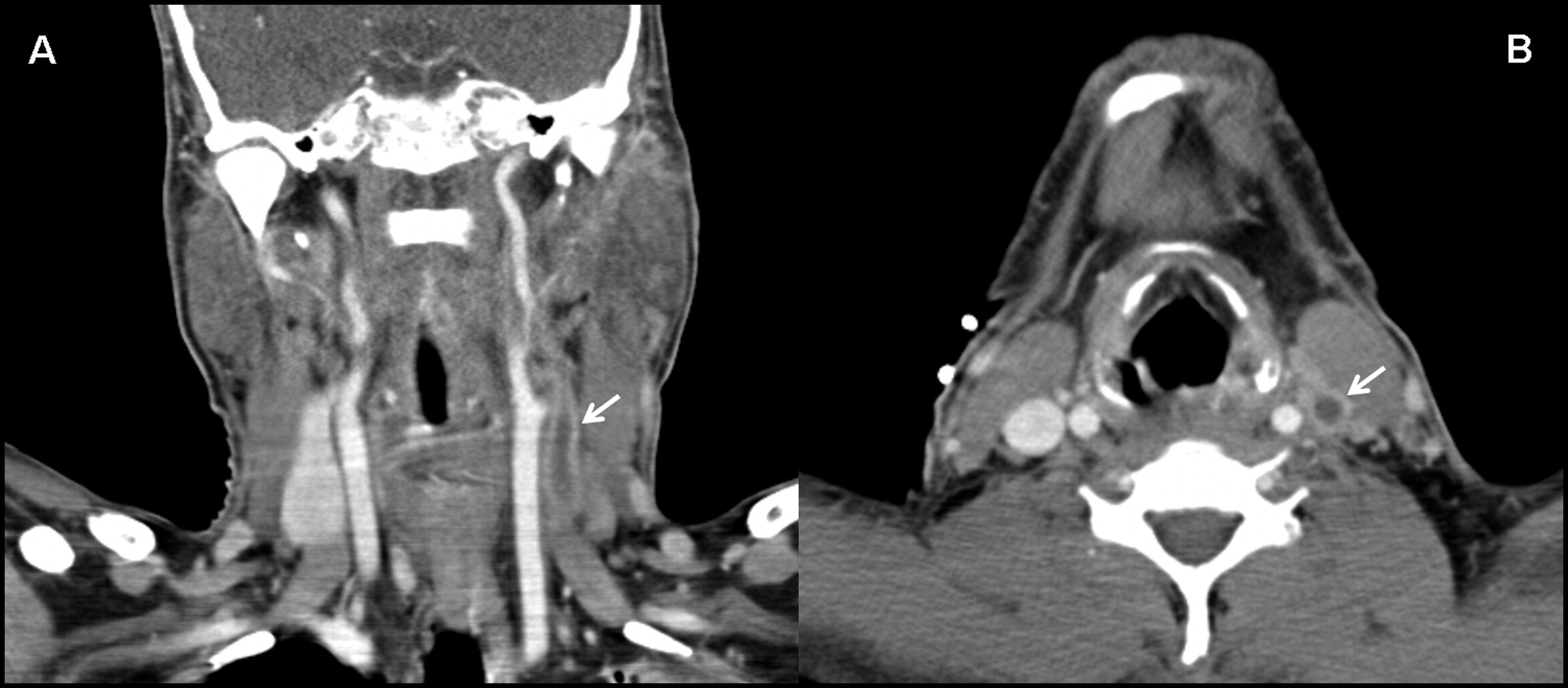
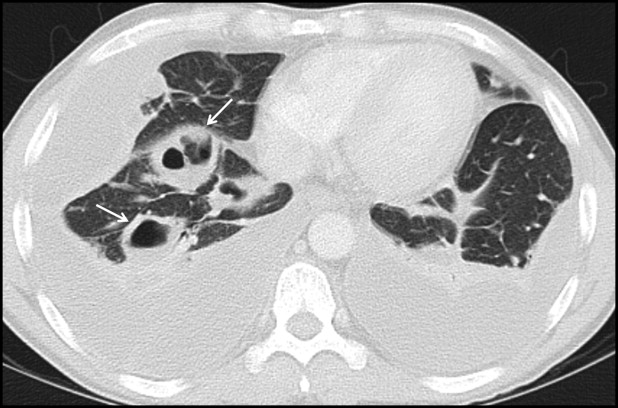
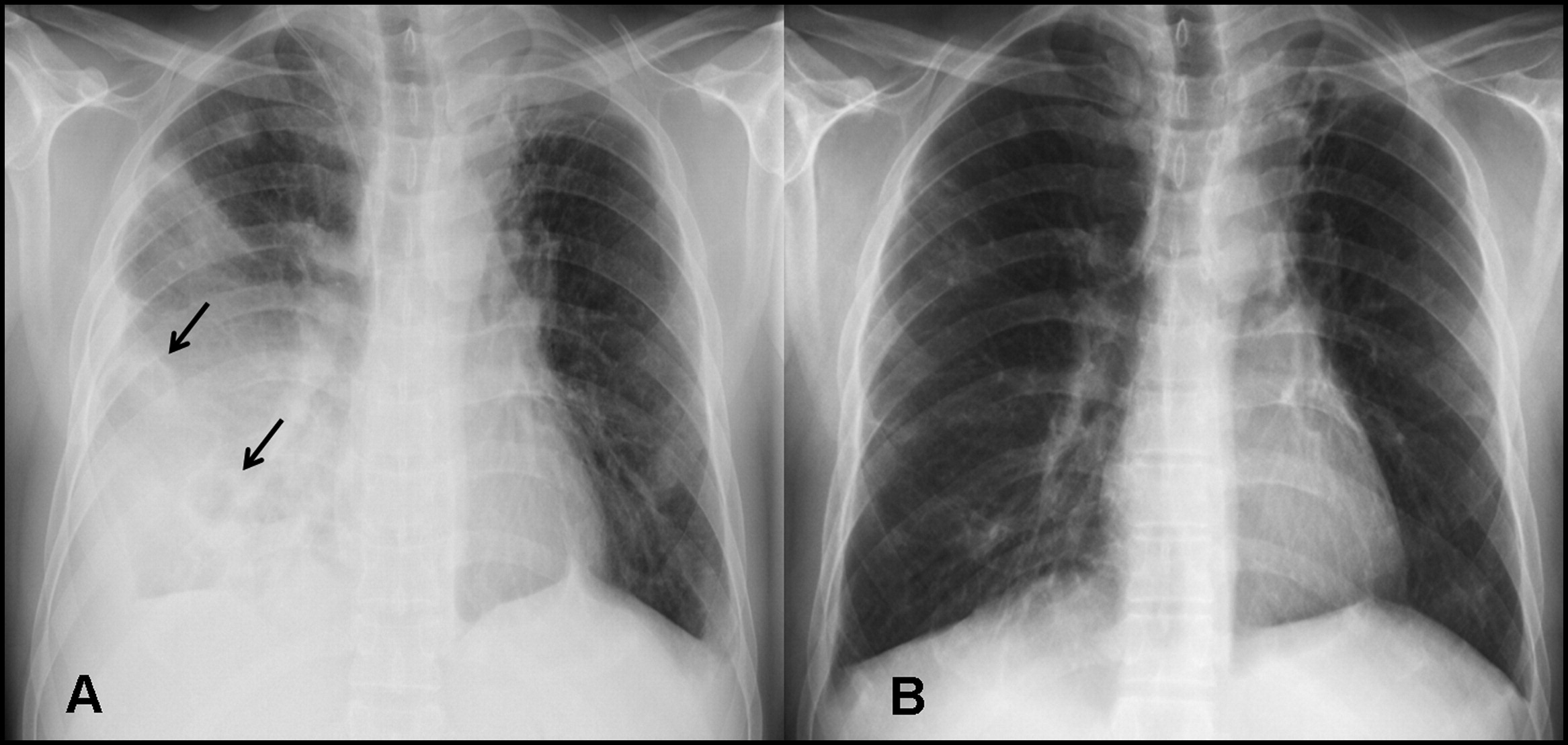
ชายอายุ 39 ปี มีไข้หนาวสั่น เจ็บคอ ไอ เหนื่อยมากขึ้นมา 1 สัปดาห์, BP 80/60, RR 45/minชายอายุ 39 ปี ไม่มีงานทำ ไม่มีบ้าน อาศัยอยู่กับเพื่อน มาที่ห้องฉุกเฉินเพราะมีไข้หนาวสั่นมา 1 สัปดาห์ ร่วมกับเจ็บคอ ไอ เหนื่อยมากขึ้น เสมหะสีน้ำตาล กินอาหารได้น้อยเพราะเบื่ออาหาร ผู้ป่วยไม่มีโรคประจำตัวใดๆ สูบบุหรี่มานาน (27 pack years) และยังสูบบุหรี่อยู่ ดื่มสุรามาตลอด PE At presentation, fever, 40.3°C; blood pressure, 80/60 mm Hg; pulse rate, 140 beats per minute; and respiratory rate, 45 breaths per minute. The submandibular and anterior cervical lymph nodes were enlarged and tender to palpation, and the inspection of the oral cavity revealed an enlargement of the left peritonsillar region with displacement of the uvula to the right. On lung auscultation, predominantly right-sided rales were found; there was no cardiac murmur. 1. ปัญหาแลละการวินิจฉัยคืออะไร 2. จะ manage อย่างไร Posted by : cpantip , E-mail : (chpantip@gmail.com) , Date : 2014-10-23 , Time : 13:00:07 , From IP : 172.29.3.50 |
|
Problem list 1 septic shock with acute respiratory failure Source ) deep neck infection ) lt peritonsillar abcess + pneumonia Mx On et tube+ mechanical ventilator Resuscitation Empiric atb ) ceftriazone + clindamycin cover gram + /- anaerobes ( community setting) ขอ ct. Head and neck confirm location + extension Consult ent for adequate drainage ครับ Posted by : Aekkamon1 , E-mail : (accumulate1985 @gmail.com) , Date : 2014-10-23 , Time : 19:14:32 , From IP : cache100.kku.ac.th |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}