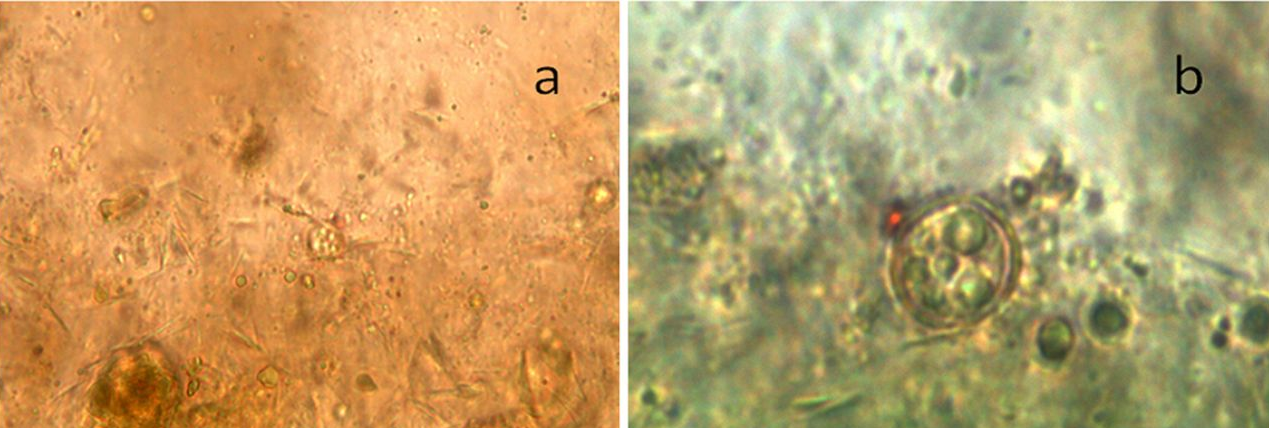
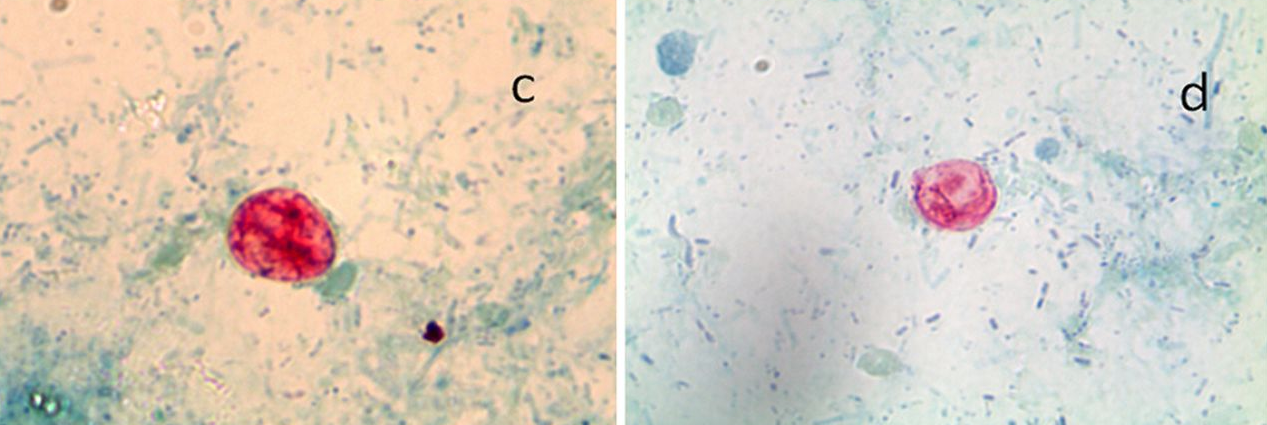
ชายอายุ 43 ปี ถ่ายอุจจาระเป็นน้ำมา 15 วันชายอายุ 43 ปี มาพบแพทย์เนื่องจากถ่ายอุจจาระเป็นน้ำมา 15 วัน ร่วมกับเบื่ออาหาร (น้ำหนักลดไป 3 กิโลกรัมใน 10 วัน) มีลมในท้องและปวดบิดเป็นครั้งคราว คลื่นไส้ และมีไข้ต่ำๆ. แพทย์ได้ส่งตรวจอุจจาระเพื่อหาพยาธิและไข่พยาธิ และเพาะเชื้อแบคทีเรีย ผลออกมาปกติ. เนื่องจากผู้ป่วยยังถ่ายอุจจาระเหลวอยู่ตลอด แพทย์จึงรับผู้ป่วยเข้าโรงพยาบาลเพื่อ investigation ต่อไป. การตรวจร่างกายแรกรับ: อยู่ในเกณฑ์ปกติ ผู้ป่วยไม่มี signs ของ dehydration และไม่มี. evidence ของ systemic infection. Lab: He had isolated monocytosis (1,300 cells/μl) with normal renal, hepatic, and pancreatic functions. -Thyroid hormone and allergologic evaluations : no abnormality. -The results for the classic parasitic serology examinations performed on travelers were negative, including the results for filariasis, strongyloidiasis, anisakiasis, ascariasis, distomatosis, trichinosis, toxocariasis, and bilharzia. Gastroesophageal endoscopy : a peptic erosive esophagitis (level 2) unrelated to the symptoms. -Small bowel biopsy specimen and a new series of three fresh stool samples were cultured for common enteropathogens (Salmonella, Shigella, Campylobacter, and Yersinia spp.) : negative results. -Ova-and-parasite exam was โดยทำ concentration และ centrifuge stool specimen. The first microscopic examination involved direct wet smears with normal microscopy (magnifications, ×200 and ×400) (Fig. 1a) for detection of single-cell parasites and worms. Some structures were observed and were more evident following oil immersion (magnification, ×1,000) (Fig. 1b). Wet stool preparations viewed using a fluorescence microscope with UV illumination showed fluorescent spherical bodies. Posted by : cpantip , E-mail : (chpantip@gmail.com) , Date : 2014-06-02 , Time : 10:02:33 , From IP : 172.29.3.129 |
 ขอโทษค่ะ ลงรูปสลับกัน Posted by : cpantip , Date : 2014-06-02 , Time : 10:06:57 , From IP : 172.29.3.129 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}