หญิงอายุ 27 ปี ทำงานเป็นพนักงานเสิร์ฟในร้านอาหาร
Problem
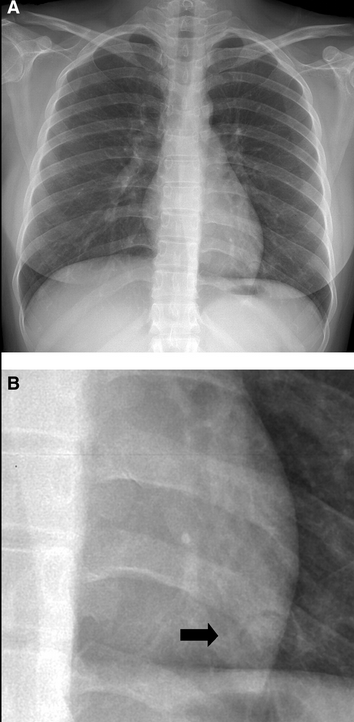
1. Hemoptysis 6 mo.
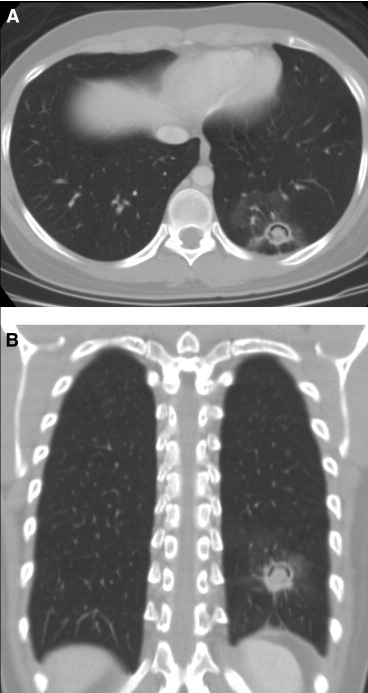
2. CXR: a mass with halo sign at LLL
3. Active smoking
Halo sign - chest
(Dr Yuranga Weerakkody and Dr Frank Gaillard et al.
http://radiopaedia.org/articles/halo-sign-chest-2)
The halo sign in chest imaging is a feature seen on lung window settings (typically HRCT), ground glass opacity surrounding a pulmonary nodule or mass and represents haemorrhage. It is typically seen in angioinvasive aspergillosis.
Other entities that may give a halo sign include
Infectious disease
• fungi -
o pulmonary aspergillosis
o pulmonary mucormycosis
o pulmonary coccidoidomycosis
o pulmonary cryptococcosis
o pulmonary candidiasis
• septic embolism
• mycobacterial -
o pulmonary tuberculosis
o pulmonary Mycobacterium avium complex infection
• rickettsia - Coxiella burnetti
• viral - herpes simplex virus, varicella zoster virus, cytomegalovirus,
myxovirus
Neoplasia
• primary tumours -
o squamous cell carcinoma of lung
o Kaposi sarcoma
o bronchioalveolar carcinoma - adenocarcinoma of lung
• lung metastasis - angiosarcoma, choriocarcinoma, osteosarcoma,
melanoma, hydatidiform mole, metastasis from GI malignancy
Non-neoplastic, non-infectious, inflammatory diseases
• Wegener granulomatosis
• eosinophilic lung disease
• pulmonary endometriosis
• organizing pneumonia
• hypersensitivity penumonitis
• iatorgenic injury
• pulmonary pseudoaneurysm
จาก CXR Halo sign เข้ากับ angioinvasive aspergillosis มากที่สุด แต่ไม่เข้ากับ clinical setting ของผู้ป่วยรายนี้ เพราะไม่ได้เป็น immunocompromise host และอาการผู้ป่วย benign มาก ไม่มี constitution symptom เลย
ผู้ป่วยรายนี้ น่าจะมี infection จากเชื้อที่ทำให้เกิดการติดเชื้อแบบเรื้อรัง เช่น
-Bacteria : TB, NTM, Burkholderia pseudomallei, Nocardia, actinomyces
-Fungus : Cryptococcus spp.
-Parasite : Paragonimiasis
นอกจากนี้ จะต้องถามประวัติว่า hemoptysis สัมพันธ์กับการมีระดูหรือไม่ (pulmonary endometriosis)
Plan: 1. HIV antibody
2. Sputum for- acid fast stain and modified acid fast stain, Gram
stain, GMS
- culture for aerobic and anaerobic bacteria,
mycobacteria, fungi
3. HRCT chest เพื่อให้เห็นรายละเอียดของรอยโรค
4. อาจต้องทำการผ่าตัดเอา lesion ออกเพื่อ definite diagnosis และเพื่อรักษาด้วย
Posted by : lara , Date : 2014-03-31 , Time : 12:23:49 , From IP : 172.29.3.141
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}