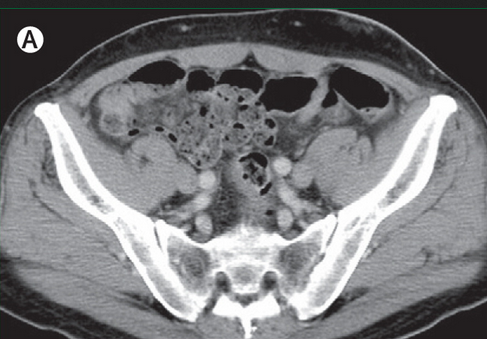
 Imaging-negative psoas abscess (A) No abnormal findings on enhanced CT on day of admission. Posted by : cpantip , Date : 2014-02-03 , Time : 12:22:42 , From IP : 172.29.3.164 |
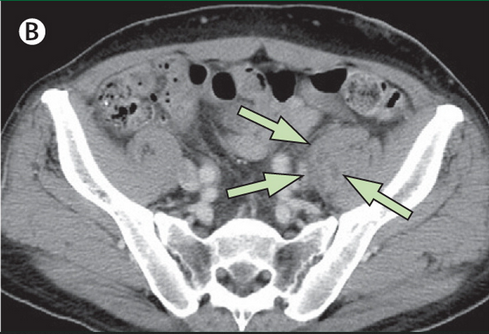
A 55-YOM on hemodialysis had acute-onset LLQ abdominal pain for 12 h.ชายอายุ 55 ปีมาตรวจที่ห้องฉุกเฉินเนื่องจากปวดที่ท้องส่วนล่างข้างซ้ายแบบ acute onset มา 12 ชั่วโมง. ผู้ป่วยรับการทำ haemodialysis มา 20 ปีเนื่องจากมี diabetic nephropathy. ผู้ป่วยปวดน้อยลงเมื่อนอนหงายโดยงอเข่าข้างซ้าย On examination, his temperature was 37.8°C and other vital signs were normal. The patient dragged his left leg when walking. The left lower quadrant of the abdomen was tender and the psoas sign (pain on hip extension) was positive on the left. CBC: white cell count ปกติ, แต่ C-reactive protein สูงเล็กน้อย. แพทย์นึกถึง psoas abscess แต่ enhanced CT และ plain MRI ไม่พบรอยโรคใดๆ. 1. การวินิจฉัยน่าจะเป็นอะไร 2. จะ manage อย่างไร Posted by : cpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2014-01-31 , Time : 13:00:11 , From IP : 172.29.3.164 |
|
Imaging-negative psoas abscess (A) No abnormal findings on enhanced CT on day of admission. Posted by : cpantip , Date : 2014-02-03 , Time : 12:22:42 , From IP : 172.29.3.164 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}