{kind=link}
{kind=link}
{kind=link}
{kind=link}
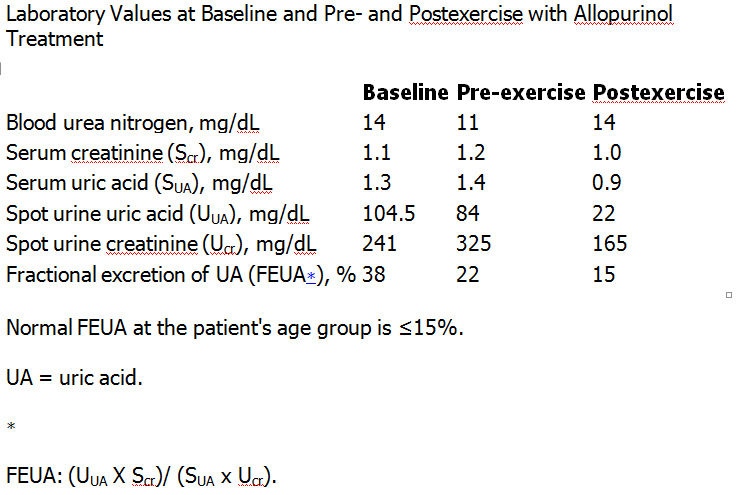 Laboratory Values at Baseline and Pre- and Postexercise with Allopurinol Treatment Posted by : cpantip , Date : 2014-01-08 , Time : 10:47:36 , From IP : 172.29.3.79 |
ชาย 18 ปี อาเจียนหลายครั้งและปวดที่เอวมากหลังจากวิ่งแข่งขัน 400 เมตร.ชายอายุ 18 ปีซึ่งแข็งแรงดีมาก่อน มาตรวจที่แผนกฉุกเฉินเนื่องจากมีอาเจียนหลายครั้งและปวดที่เอวมากหลังจากวิ่งแข่งขัน 400 เมตร. ผู้ป่วยมีอาการเช่นนี้มาก่อนเมื่อ 3 เดือนก่อนหน้านี้ ไม่มีประวัติไข้หรือมีการติดเชื้อที่ใดมาก่อนหน้านี้ ไม่มีปวดเมื่อยกล้ามเนื้อ ไม่มีชัก ปัสสาวะสีปกติ ไม่เคยใช้ยาเสพติดใดๆ Initial laboratory assessment in the Emergency Department showed: blood urea nitrogen 28 mg/dL, creatinine 3.4 mg/dL, and serum uric acid (UA) 1.5 mg/dL; serum myoglobin, creatinine kinase, and aldolase were normal. Urinalysis was unremarkable. 1. การวินิจฉัยคืออะไร 2. จะ manage อย่างไร Posted by : cpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2014-01-05 , Time : 13:51:38 , From IP : 172.29.3.79 |
|
Laboratory Values at Baseline and Pre- and Postexercise with Allopurinol Treatment Posted by : cpantip , Date : 2014-01-08 , Time : 10:47:36 , From IP : 172.29.3.79 |
{kind=link}
{kind=link}