ความคิดเห็นทั้งหมด : 6
เด็กชายอายุ 4 เดือน มีไข้และ stiff neck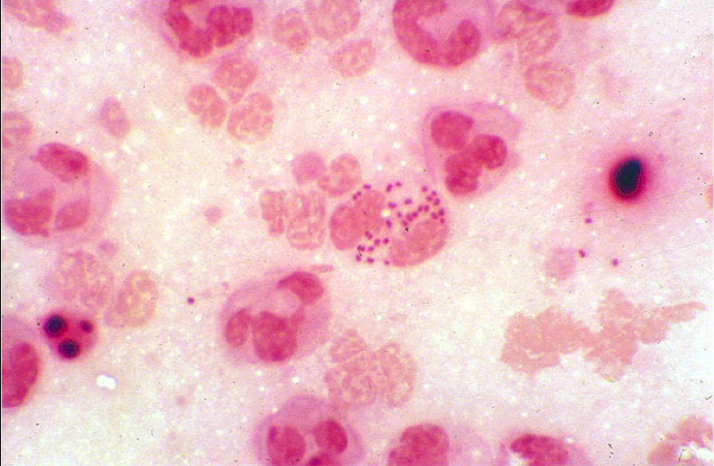 เด็กชายอายุ 4 เดือนซึ่งแข็งแรงดีมาก่อนถูกนำส่งโรงพยาบาลเนื่องจากมีไข้ ร้องกวนตลอด แพทย์ตรวจพบว่าผู้ป่วยมี stiff neck และ Brudzinski sign positive. Cerebrospinal fluid (CSF) : WBC 2500/cu mm, 57% neutrophils, and high protein (1.6 g/L). • Gram stain ของ CSF ดังรูป 1. การวินิจฉัยคืออะไร 2. จะ manage อย่างไร Posted by : cpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2013-05-05 , Time : 15:10:52 , From IP : 172.29.3.216 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}