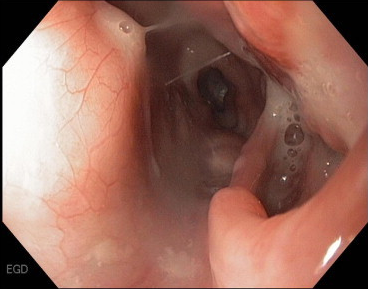
รูป Spontaneous esophageal perforation in a patient with tuberculosis.
Esophagogastroduodenoscopy: A large esophageal perforation near an area of thickened mucosa (รูปi). . Biopsies ที่ thickened mucosa พบเชื้อ acid fast bacilli และเพาะเชื้อขึ้น Mycobacterium tuberculosis. Ascites culture ก็ขึ้น M. tuberculosis. ผู้ป่วยได้รับการทำ esophageal stenting ซึ่งได้ผลดี และได้รับอนุญาตให้กลับบ้านหลังเริ่มการรักษาด้วยยาต้านวัณโรค HRZE.
M. tuberculosis เป็น acid-fast bacillus ซึ่งส่วนใหญ่แล้วทำให้เกิดโรคที่ปอด แต่เชื้อนี้สามารถ ทำให้เกิดการติดเชื้อที่อวัยวะต่างๆ เช่น central nervous, skeletal, genitourinary, และ gastrointestinal systems. ข้อมูลจาก US CDC ในปี 2010 มีผู้ป่วย 11,182 ราย (3.6 รายต่อ 100,000), และประมาณ 1/3 มี extrapulmonary TB.
อาการของ gastrointestinal tuberculosis ไม่จำเพาะ โดยผู้ป่วยมีอาการ anorexia, nausea, vomiting, abdominal pain, fevers, constipation, diarrhea, rectal bleeding, และ weight loss ซึ่งทำให้แพทย์วินิจฉัยได้ล่าช้าและมีความเสี่ยงในการแพร่กระจายสู่ผู้อื่น. Intraluminal involvement ของ M. tuberculosis เป็นได้ตั้งแต่ mucosal inflammation จนถึงsevere ulceration และสามารถทำให้สับสนกับ Crohn”s disease และมะเร็งเช่น carcinoma หรือ lymphoma. Chronic infection สามารถทำให้เกิด fibrosis และที่พบน้อยกว่า คือ perforation. Perforation บางครั้งเกิดจากการลุกลามโดยตรงจากตำแหน่งที่มีการติดเชื้ออีกแห่งหนึ่ง เช่น ต่อมน้ำเหลือง. แม้ว่า surgical repair เป็นการรักษาสำหรับ colonic หรือ enteric perforation, แต่มี paradigm shift สำหรับการรักษา esophageal perforation ด้วย esophageal stenting. แม้ว่าจะมีความเสี่ยงของ perforation, pain, stent migration และdysphagia ผู้ป่วยก็มักจะทนต่อ esophageal stents ได้ดี และทำให้รูรั่วหายถึง 85% ของผู้ป่วยจากสาเหตุต่างๆ.
Reference: Joseph G. Baltz JG, et al. Esophageal perforation caused by Mycobacterium tuberculosis. Am J Med 2013;126:e5-6.
Posted by : cpantip , Date : 2013-04-25 , Time : 12:15:56 , From IP : 172.29.3.216
|
{kind=link}
{kind=link}
{kind=link}