มีรายงาน cutaneous amebiasis ครั้งแรกเมื่อปี 1892 โดย Nasse รายงานผู้ป่วย amoebic liver abscess ซึ่งมีภาวะแทรกซ้อนหลังการระบายหนอง เกิดมี extensive ulceration และ necrosis ของ abdominal skin, subcutaneous tissue และ muscles. cutaneous amebiasis เป็น clinical form ที่พบน้อยที่สุดของ human amebiasis และโดยทั่วไป เป็นผลเนื่องมาจากการติดเชื้อ Entamoeba ของผิวหนังที่มีความเสียหายมาก่อน. Ngai และ Frazier ทบทวนรายงานที่ตีพิมพ์ก่อนปี 1936 พบว่ามีรายงาน 27 รายจากจีน, Indochina, และสหรัฐอเมริกา. หลังจากนั้น จำนวนผู้ป่วย cutaneous amebiasis ที่รายงานลดลงเป็น 11 รายในปี 1941. Magaña และคณะรายงาน 26 documented cases ของ cutaneous amebiasis จาก clinical files ของ Pediatric Dermatology Department of the General Hospital of Mexico of the Health Ministry, และจาก Pathology Department ของ Hospital of Medical Specialties of the Mexican Institute of Social Security (IMSS). อย่างไรก็ตาม ส่วนใหญ่ของผู้ป่วยรายงานในช่วงปี 1969 - late 1980s. ผู้ป่วยเหล่านี้มี deep skin lesions ที่ anal, perineal, vulval, vaginal และ genital regions, เช่นเดียวกับ diaper area ของทารกที่มีท้องเสียจาก Entamoeba histolytica. ในผู้ใหญ่ ตำแหน่งของ cutaneous amebiasis ที่พบบ่อยคือ abdominal area ซึ่งเกิดจาก involvement ของ abdominal wall ระหว่างที่มี spontaneous amoebic liver abscess หรือเป็นภาวะแทรกซ้อนจากการระบายหนอง amoebic liver abscess. การติดต่ออีกทางหนึ่งของ cutaneous amebiasis คือการร่วมเพศ.
รายนี้แสดงถึง sexually transmitted genital cutaneous amebiasis และเน้นความสำคัญของ clinical form นี้ ของ amoebic disease ซึ่งแม้ว่าจะพบ cutaneous amebiasis ได้น้อย แต่ก็ต้องเป็น differential diagnosis ของ ulcerative lesions ของ human genitalia, โดยเฉพาะอย่างยิ่งใน amebiasis-endemic areas และใน high risk groups. การวินิจฉัยให้ทันการ และการรักษาให้ตรงโรคมีความสำคัญในการป้องกัน serious anatomical damage และรอยโรคหายโดยไม่มี functional sequelae.
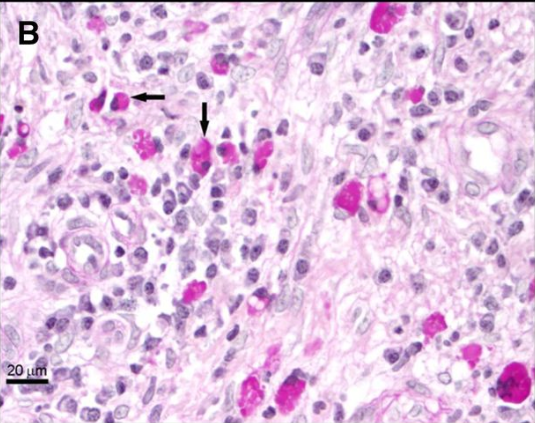
Ref: Morán P, et al. Cutaneous amebiasis: the importance of molecular diagnosis of an emerging parasitic disease.Am J Trop Med Hyg 2013;88: 186-190.
Posted by : cpantip , Date : 2013-03-07 , Time : 15:26:00 , From IP : 172.29.3.93
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}