ความคิดเห็นทั้งหมด : 3
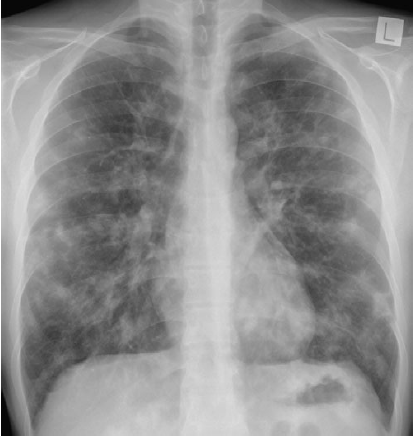
A 28-YOM had a pruritic, erythematous rash on his trunk, buttock and legs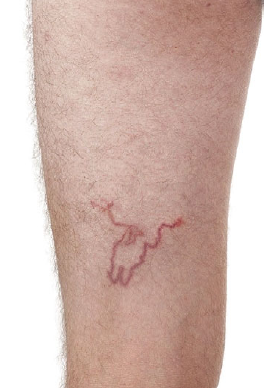 ชายอายุ 28 ปีมาตรวจที่แผนกฉุกเฉินเนื่องจากมีผื่นแดงคันที่หลัง ลำตัว ก้น อวัยวะเพศ และขาทั้งสองข้าง. (รูป 1 และ 2). ผื่นนี้ปรากฎมาได้ 1 เดือนโดยเริ่มเป็นที่ก้นก่อน ผู้ป่วยได้ใช้ทั้งยาทาและยากิน steroids, antihistamines, antibiotics, และ permethrin แต่อาการก็ไม่ดีขึ้น. 2 สัปดาห์ก่อน ผู้ป่วยเริ่มมีไอแห้งๆ และหายใจมีเสียงวี๊ด. ผู้ป่วยเบื่ออาหารและน้ำหนักลดไป 3กก. ใน 1 เดือน Posted by : cpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2012-06-28 , Time : 12:59:23 , From IP : 172.29.3.13 |

{kind=link}
{kind=link}
{kind=link}
{kind=link}