ชายอายุ 45ปี มีปัญหา
1. ไข้ เจ็บหน้าอกตรงกลางอกและซึมลงมา 5 วัน.
2. เป็นชาวนา ชำแหละวัวที่ตายเมื่อ 8 วันก่อนเริ่มไม่สบาย.
3. fever, shock, a painless ulcerative skin lesion on the right hand and meningeal signs.
CXR: Widening of mediastinum, cardiomegaly?, prominence of both hilar with perihilar infiltration. bilat pleural effusion?
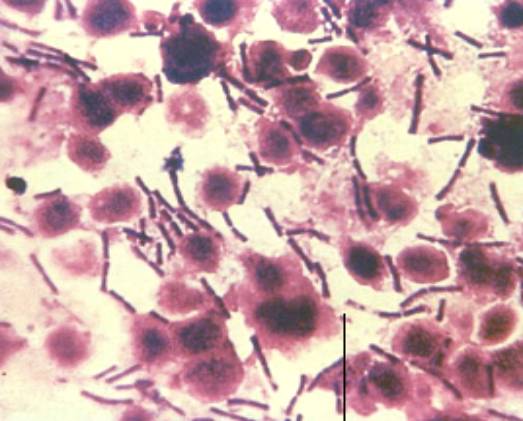
สรุปว่าผป.มี skin lesion ที่มือหลังชำแหละวัวตาย มีไข้, pneumonia with widening mediastinun และ meningitis เชื้อก่อโรคน่าจะเป็น Bacillus anthracis มากที่สุด
Management
1. Blood culture, pus swab culture (ทำ gram stain ด้วย).
2. LP ดู cell, glucose, protein, ย้อมสีแกรม และเพาะเชื้อ
การรักษา: B. anthracis is highly susceptible to a variety of antimicrobial agents including penicillin, chloramphenicol, tetracycline, erythromycin, streptomycin, and fluoroquinolones. B. anthracis is NOT susceptible to cephalosporins or trimethoprim-sulfamethoxazole. (จาก UpToDate)
ควรให้ high dose of penicillin + ciprofloxacin IV.
Posted by : lara , Date : 2012-04-26 , Time : 14:45:06 , From IP : 172.29.3.14
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}