ความคิดเห็นทั้งหมด : 14
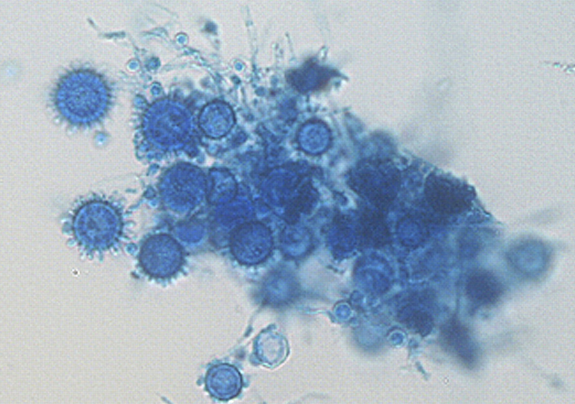
A 31-YOM had fever, abdominal pain and gingival lesion. ชายอายุ 31 ปีมีไข้และปวดทั่วท้องมา 5 วัน. ผู้ป่วยมีรอยโรคที่เหงือกและบวมๆ ที่คอซึ่งไม่เจ็บมา 1 เดือน อ่อนเพลียและเบื่ออาหารมา 3 เดือน. น้ำหนักลดไป 10 กก. ผู้ป่วยทำงานก่อสร้าง. Physical examination revealed oral candidiasis, granulomatous gingiva (รูป 1), multiple palpable left supraclavicular and cervical lymph nodes (the largest up to 3.0 × 2.5 cm2, and hepatosplenomegaly. Laboratory investigation revealed -CBC: WBC 5,800 cell/cu mmL with 91% neutrophils and 4% lymphocytes, hemoglobin level of 11.2 g/dL, a platelet count of 180,000 cells/cu mm 1. การวินิจฉัยที่น่าจะเป็นคืออะไร 2. จะ manage อย่างไร Posted by : cpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2012-02-17 , Time : 15:45:43 , From IP : 172.29.3.68 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}