ขอบคุณคุณหมอ Kenny มากค่ะlesiy[8e9v[
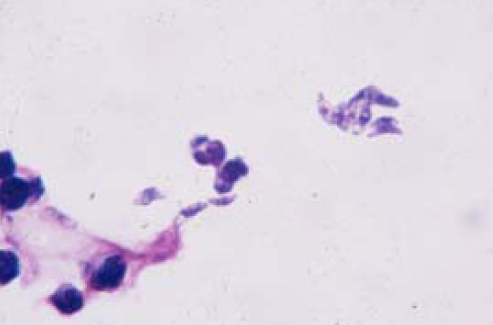
เชื้อก่อโรคของ pneumonia ในผู้ป่วย post renal transplant ที่สำคัญคือ Pneumocystis jiroveci, CMV และ toxoplasma. ในรูป BAL ของผู้ป่วย พบเชื้อที่เป็นรูปพระจันทร์เสี้ยว ซึ่งเป็นลักษณะของ Toxoplasma gondii.
ช่วงหลังทำ transplantation ผู้ป่วยมีความเสี่ยงต่อการเกิด opportunistic infection หลายอย่าง เนื่องจากการรักษาระยะยาวด้วย immunosuppressive agents เช่น cyclosporine และ tacrolimus ซึ่งทำให้สูญเสีย cellular immunity . T. gondii เป็น opportunistic pathogens ที่พบบ่อยตัวหนึ่งในผู้ป่วยกลุ่มนี้ และเชื้อนี้สามารถทำให้เกิด clinical syndromes ได้หลายแบบ. ใน solid organ transplant (SOT) recipients ซึ่งรวมถึง renal transplantation ส่วนใหญ่ของ toxoplasmosis เกิดจากการแพร่ของเชื้อ protozoa นี้ที่อยู่อย่างสงบใน transplanted organ ของ Toxoplasma-seropositive donor ไปสู่ Toxoplasma-seronegative recipient.
Toxoplasmosis มักเกิดขึ้นภายใน 3 เดือนหลัง transplantation, โดยอาจมีfebrile myocarditis, encephalitis, pneumonitis และ disseminated infection. การวินิจฉัย toxoplasmosis ขึ้นอยู่กับการตรวจพบเชื้อนี้หรือ DNA ของเชื้อนี้ในเลือด, bone marrow, cerebrospinal fluid, bronchoalveolar
lavage fluid, หรือ biopsy specimen อื่นๆ. Serological tests ไม่มีประโยชน์ในการวินิจฉัยเพราะมีอัตราสูงของผล false negative และ false positive.
สำหรับการป้องกัน toxoplasmosis, serological screening ของ donors และ recipients ก่อน transplantation ทำให้สามารถระบุผู้ป่วยที่มีความเสี่ยงสูงของ toxoplasmosis, เช่น seropositive hemopoietic stem cell transplant (HSCT) recipients และ mismatched (seropositive donor/seronegative recipients) SOT recipients. Co-trimoxazole เป็น drug of choice สำหรับ primary chemoprophylaxis ของ toxoplasmosis. สำหรับการรักษา ให้ co-trimoxazole นาน 4-6 สัปดาห์ และตามด้วยsecondary prophylaxis จนกระทั่งมี recovery ของ immune status.
Reference: Mootsikapun P. A 40-year-old man, with a history of renal transplantation, presented with subacute progressive dyspnea for 2 weeks. JIDAA 2009; 26:61, 75.
Posted by : cpantip , Date : 2012-02-17 , Time : 15:36:16 , From IP : 172.29.3.68
|
{kind=link}
{kind=link}
{kind=link}