1. Dyspnea caused by Heart Lung Metabolic and Psychogenic
2. Physical examination revealed distention of the jugular veins ทำให้คิดถึงสาเหตุจาก Heart มากที่สุด แต่จะต้องดู Wave form ของ JVP ด้วยครับเพราะมีประโยชน์มากในการวินิจฉัยโรค เช่น
A.กลุ่มไม่พบ wave form เช่น Superior vena cava syndrome
B.กลุ่ม normal wave form เช่น Bradycardia Fluid overload Heart Failure
C.กลุ่ม Abnormal wave form เช่นGiant a wave อาจจะมากจาก Heart failure, PS, Pulmonary hypertension,Tricuspid stenosis(with slow y descent). Cannon a wave ส่วนมากจะมาจาก complete heart block, prematurity, ventricular rhythm, atrial flutter.Large v with Rapid vy เกิดใน Tricuspid regurgitation.Absence a wave atrial fibrillation.Kussmaul with slow y descent เจอใน pericardial effusion, constrictive pericarditis,cardiac tamponade
โดยผมขออธิบายลักษณะของ JVP ปรกติคร่าวๆครับว่า JVP ปรกติของคนเรานั้นมี wave form ตามการบีบตัวของหัวใจครับ ได้แก่ a wave เป็น positive wave เกิดจาก atrial contraction. c wave เป็น small positive wave ที่เกิดจาก ventricular isovolumetric contraction แล้วกระทบ atrioventricular valve ส่งเป็นแรงเข้าสู่ atrium. x wave เป็น negative wave ที่เกิดจาก atrial relaxation. v wave เป็นที่เกิดจาก Atrial filling ตรงกับ late ventricular contraction. y wave เกิดจาก atrium ถีบเลือดเข้า ventricle
Jugular venous wave form นี้"สำคัญอย่างยิ่งในการตรวจร่างกาย" เพราะโรคบ้างโรคสามารถให้การวินิจฉัยจากการสังเกตลักษณะดังกล่าวได้ง่ายกว่าการฟังเสียอีกเช่น Tricuspid regurgitation เพราะน้อยคนที่ Mann-Cavallo sign จะ positive แต่แทบทุกคนที่เห็น JVP rapid vy ได้ชัด และ JVP wave form เป็นควรรู้ที่พัฒนามานานตั้งแต่ พ.ศ. 2410 โดย Pierre Charles Édouard Potain แพทย์ชาวฝรั่งเศส ในเค้าได้ให้การสังเกตง่ายว่าการดู JVP สามารถเริ่มดูจาก x wave จะเป็นการดีที่สุดเพราะเป็น large negative wave ที่อยู่ระหว่าง S1 และ S2 พอดี เมื่อได้ x wave แล้วการหา wave ข้างเคียงก็ไม่ใช่เรืองยาก
3.การตรวจไม่พบ murmur หรือ abnormal heart sound ทำให้คิดว่าต้นเหตุไม่ควรอยู่ที่ valve wall or myocardium จึงคิดถึง pericardium มากที่สุดครับ แต่อย่างไรก็ตามการตรวจร่างกายที่ดีสามารถบอกถึง pericardium ได้ครับ โดยให้ผู้ป่วยนั่ง หรือ นอนตะแคงซ้ายแล้วฟังที่ Apex จะได้ลักษณะของ distant heart sound ครับ
4.enlarged left cervical lymph node.จะต้องหา มะเร็งหรือติดเชื้อ(Lung และ GI) เพราะอาจจะเป็นสาเหตุที่ทำให้เกิด pericardial effusion ได้ครับ สำหรับ infection นานๆจะต้องระวัง Mycobacterium tuberculosis และ burkholderia pseudomallei ด้วยนะครับ พวงนี้มักจะมี pericarditis ร่วมด้วย
5.Investigation ควรทำ EKG ควรหา low QRS voltage เพื่อดูว่ามีน้ำในเยื่อหุ้มหัวใจหรือไม่และควรดู electrical alternan เพื่อดู tamponade ด้วยครับ นอกจากนั้นอย่างลืมดู pericarditis ด้วยซึ่งจะมี 4 ระยะครับได้แก่ Stage 1 Pericarditis Changes เห็นเป็น Diffuse concave upward ST segment elevation, ST segment depression in leads aVR or V1, Concordant T Wave changes, PR Segment depression in leads II, AVF, and V4-V6. Stage 2 Pericarditis Changes เห็นเป็น ST segment returns to baseline,T Wave flattens. Stage 3 Pericarditis Changes เห็นเป็น ST segment returns to baseline, T Wave inverts in leads II, AVF, and V4-V6.
Stage 4 Pericarditis Changes เห็นเป็น Gradual resolution of T Wave inversion.
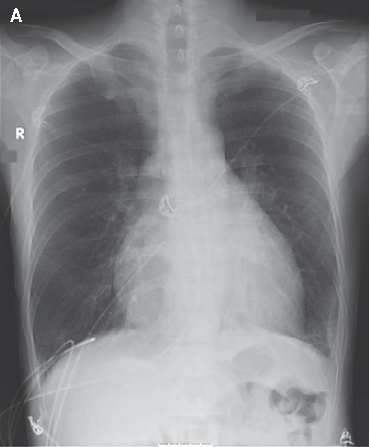
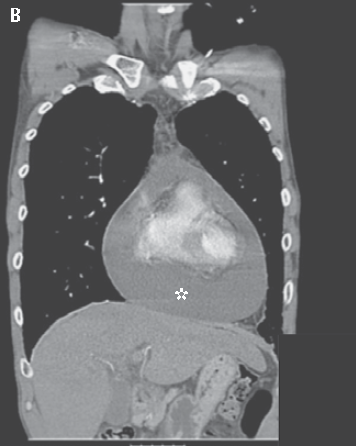
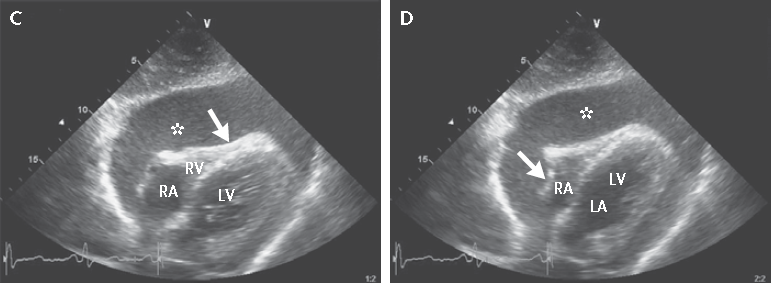
และควรทำ CXR หา "Heart โต Lung Clear" สุดท้ายก็ตัวพระเอกก็คือ Echocardiogram ควรหาน้ำใน interpericardial space ควรดูลักษณะว่ามี fibrin มากหรือไม่ ปริมาณเท่าไหร่ และมี tamponade effect หรือไม่โดยดูจาก RA-RV diastolic collapse
6.ควรทำ Lymph node biopsy เพื่อหาสาเหตุครับ
7.Observe clinical ถ้าเห็นมากอาจจะทำ pericardiocentesis ครับ
Posted by : kenny , E-mail : (Streptokinase@hotmail.com) ,
Date : 2011-11-26 , Time : 22:51:26 , From IP : 110.77.251.145
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}