 Ans Posted by : kenny , E-mail : (streptokinase@hotmail.com) , Date : 2011-09-09 , Time : 17:12:44 , From IP : 172.29.26.85 |
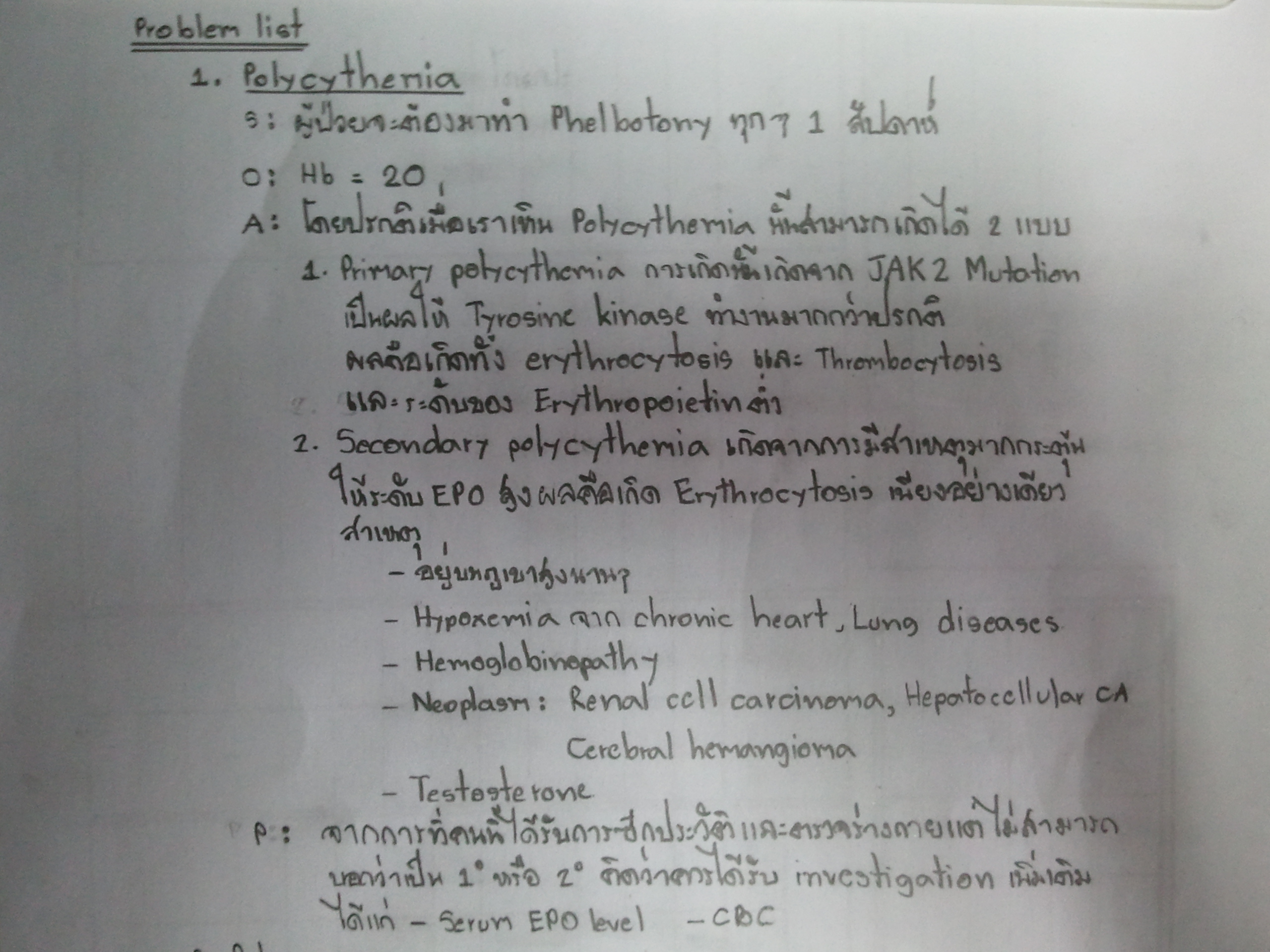
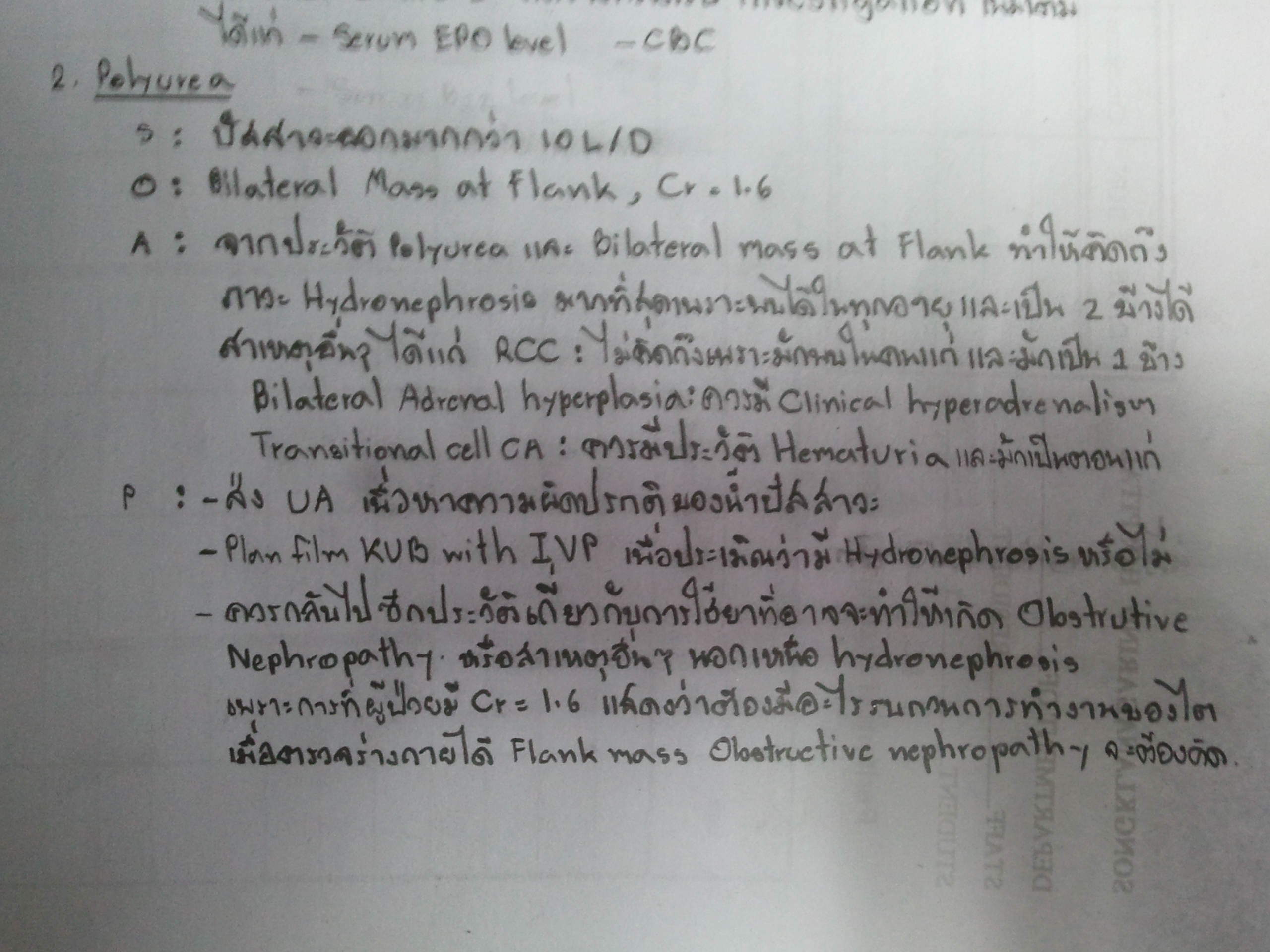
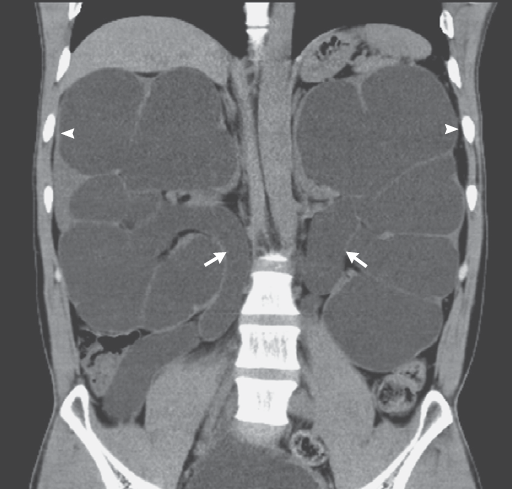
A 34-YOM had a 3-year history of polycythemia that required monthly phlebotomy.ชายอายุ 34 ปีถูกส่งมารพ.เพื่อหาสาเหตุของการมี polycythemia ซึ่งต้องทำ phlebotomy เดือนละครั้งมานาน 3 ปี. ผู้ป่วยไม่สูบบุหรี่ มีโรคประจำตัวคือ congenital nephrogenic diabetes insipidus โดยมีปัสสาวะออกประมาณ 12 - 15 ลิตรต่อวัน. Physical examination revealed euvolemia and massive, palpable kidneys. The patient showed no shortness of breath and was not hypoxic. ผล laboratory tests : hemoglobin level = 20.2 g per deciliter (N 13.5 to 18.0) และ serum creatinine level = 1.6 mg per deciliter (N 0.7 to 1.2). 1. ผู้ป่วยน่าจะมี polycythemia จากสาเหตุใด 2. จะ manage อย่างไร Posted by : cpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2011-09-08 , Time : 15:54:46 , From IP : 172.29.3.68 |
|
Ans Posted by : kenny , E-mail : (streptokinase@hotmail.com) , Date : 2011-09-09 , Time : 17:12:44 , From IP : 172.29.26.85 |
 Ans Posted by : kenny , E-mail : (streptokinase@hotmail.com) , Date : 2011-09-09 , Time : 17:13:27 , From IP : 172.29.26.85 |
 Ans Posted by : kenny , E-mail : (streptokinase@hotmail.com) , Date : 2011-09-09 , Time : 17:14:02 , From IP : 172.29.26.85 |
|
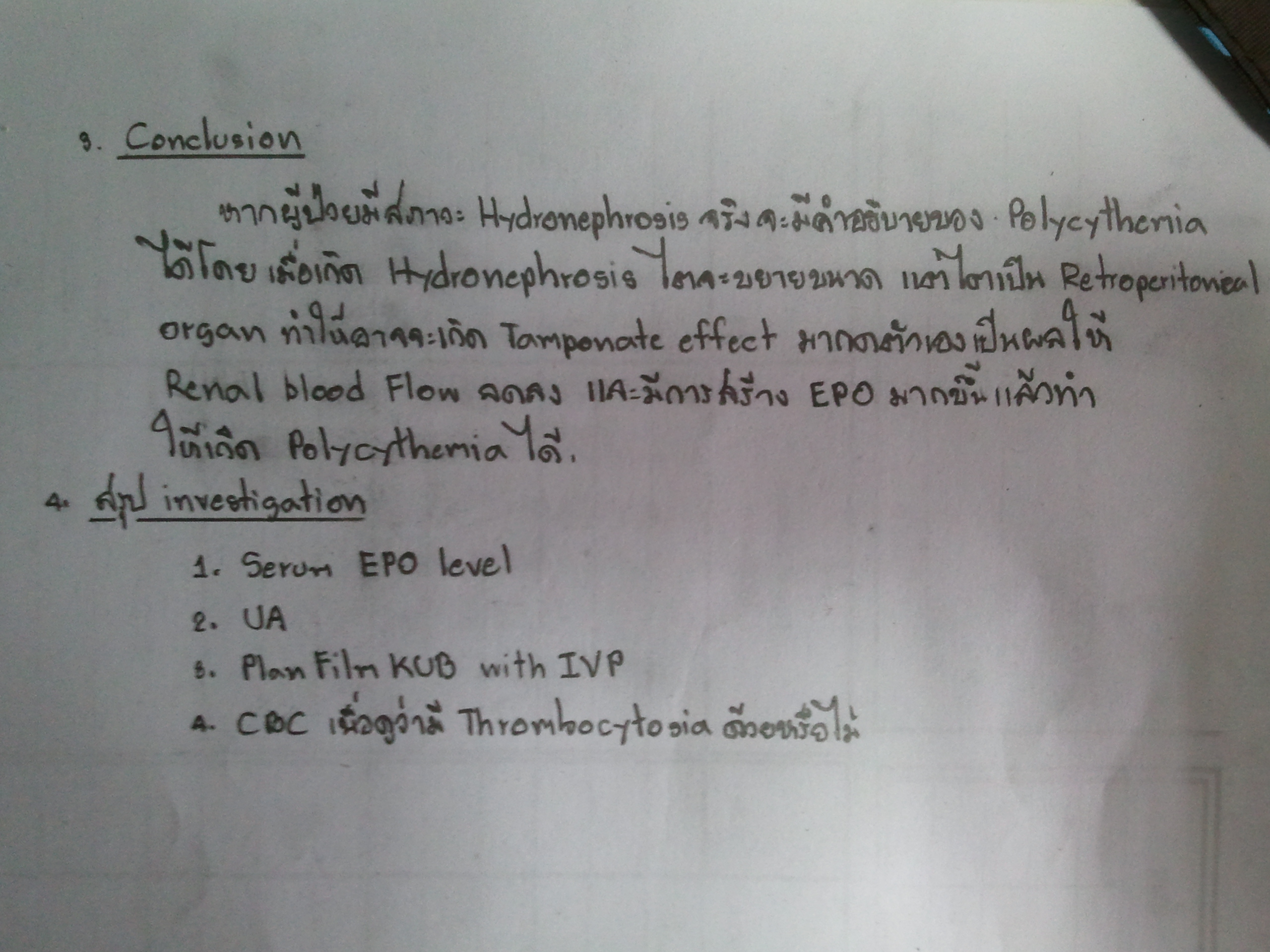
1.Bilateral hydronephrosis with hydroureter full bladder above suprapubic area อาจจะใส่ foley คาไว้ 2.จากการที่คนไข้เป็น congential nephrogenic DI แสดงว่า Arginine vasopressin ทำงานไม่ได้ จึงทำให้ Aquaporine ที่ collecting duct ไม่ทำงาน ผลคือคนไข้จะมี free water lost มาก Na ในร่างกายจะคลั่งจึงควรแนะนำให้คนไข้ ดื่มน้ำทดแทน free water ที่เสียไป และจำกัดเกลือ ถ้ายังไม่อยู่ก็ใช้ HCTZ ดึงเกลือออกร่วมด้วย 3.Phelbotomy Posted by : kenny , E-mail : (streptokinase@hotmail.com) , Date : 2011-09-13 , Time : 07:33:46 , From IP : 110.77.230.221 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}