+++ตอบไม่ถูกขอโทษนะครับอาจารย์ยังเป็น นศพ ปี4 และยังไม่ได้ขึ้น Med ที่ครับ+++
CC:หญิง 50 ปีมารพ.เนื่องจากมีไข้และสับสนมาหลังจากได้รับ fluoroquinolones มา 2 course เพื่อรักษา otitis media
S:-หญิง 50 ปี
-มีไข้และสับสนมาหลังจากได้รับ fluoroquinolones มา 2 course
-Past of otitis media
O:- fever, tachycardia, and left-sided suppurative otorrhea
- Neurologic examination demonstrated disorientation and papilledema.
-leukocytosis
-Ear fluid cultures were negative
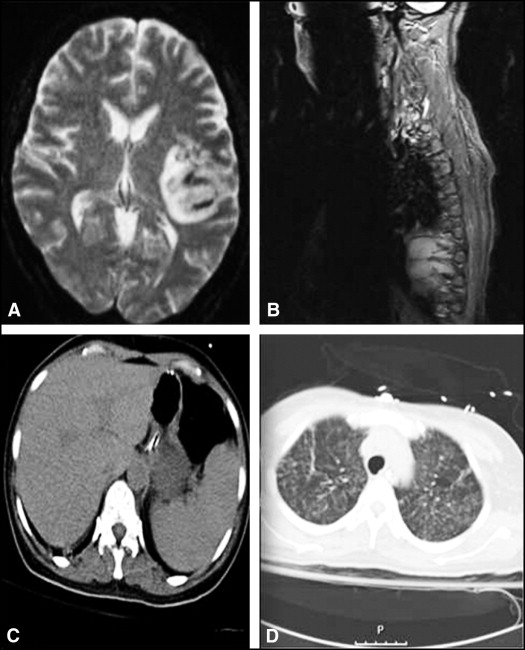
-CXR:diffuse reticulonodular infiltrates.
-CT of the head showed a mass effect .
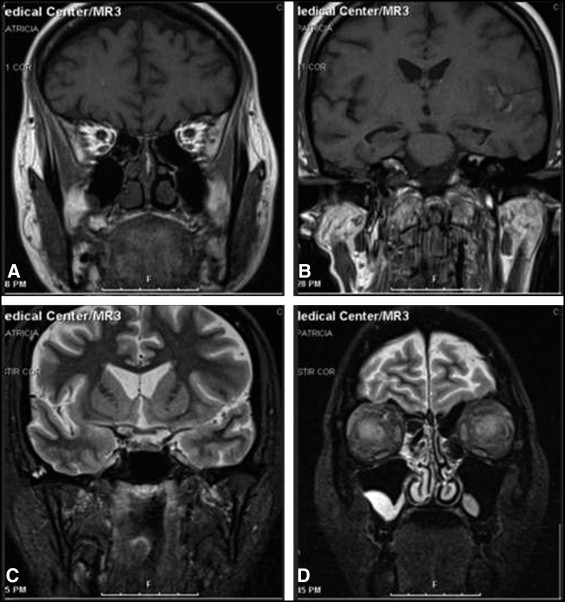
-MRI:multiple ring-enhancing lesions throughout the brain.
-MRI:of the spine identified diffuse vertebral lytic lesions.
-CT of the abdomen:hypodense lesions involving the liver and spleen
A:(clinical Part) ตอนแรก เรื่อง otitis media ทราบเกิดจาก infection Streptococcus pneumoniae Haemophilus influenzae และ Moraxella catarrhalis ตามที่ ENT สอนผมมา แต่ Lab บอกว่า Ear fluid cultures were negative จึงคิดถึงเชื้อเหล่านี้ลดลงในการใช้อธิบาย case นี้ครับ แต่ผมยังไม่ได้ตัดประเด็นของ infection ทิ้งไป แต่ผมหันไปมองกลุ่มที่มี infection ที่ทำให้เกิดอาการทาง CNS และ Pulmonary ก็เห็นl cause ที่เกิดได้ คือ 1.Toxoplasma gondii
2.Nocardiosis
3.Actinomycosis
4.Miliary tuberculosis
5.Pneumocystis jiroveci (อากการมักจะหนักไปทางปอด)
แต่ทั้งหมดมักจะพบใน immunocompromised host หรือ immunocompretent host และสามารถทำให้เกิดพยาธิสภาพที่ CNS และ Lung ได้ทั้งนั้น
(Lab part) : multiple ring-enhancing lesions throughout the brain.
เท่าทีผมทราบมันเป็นรอยโรคที่พบได้ใน MAGIC DR (จาก step up to medicine ครับ)
•Metastases(ในรายนี้ไม่พบ)
•Abscess
-pyogenic abscess and abscess caused by atypical organisms, such as bacterial pathogens (Mycobacteria, Nocardia, Actinomyces, Rhodococcus, and Listeria); fungal pathogens (zygomycosis, Histoplasma, Coccidioides, Aspergillus, and Cryptococcus); parasitic pathogens (neurocystircercosis, Echinococcus, and Entamoeba);Prorozoal(Toxoplasma)
•Glioma and other primary CNS neoplasms (ไม่พบในรายนี้)
•Infarction(ไม่พบในรายนี้)
•Contusion(ไม่พบในรายนี้)
•Demyelination (multiple sclerosis)(จะต้องพบ neuro defect แบบเป็นๆ หายๆ มากก่อน)
•Resolving hematoma/radionecrosis.(ไม่พบในรายนี้)
CXR:diffuse reticulonodular infiltrates ที่สามารถเป็นไปได้ในรายนี้
•Pneumocystis jiroveci(อากการมักจะหนักไปทางปอด)
• Miliary tuberculosis
• Nocardiosis
• Toxoplasma gondii
• Cytomegalovirus(อาการมักแสดงออกทางตา)
MRI:of the spine identified diffuse vertebral lytic lesions
คิดถึง Miliary tuberculosis Nocardiosis มากกว่า Toxoplasma gondii ซึ่งมักจะไม่ไป invade bone
ตอนนี้ที่เป็นไปได้มี สอง อย่าง
1th: Miliary tuberculosis น่าจะมีโอกาสเป็นไปได้สูงกว่าเพราะพบการลุกลามไปยังกระดูกสันหลังได้สูงกว่า และการเพราะเชื้อ จะไม่ขึ้นบน blood agar
2nd:Nocardiosis น่าจะเป็นไปได้น้อยกว่า เพราะลูกลามน้อยไปยังกระดูกสันหลังเกิดได้น้อย และสามารถเพาะเชื้อได้บน blood agar แต่โอกาสการเกิด suppulative infection น่าจะสูงกว่าครับ
Dx:ยังไงผมยังแยกไม่ออกครับ มันก้ำกึ่ง แต่เอา Miliary tuberculosis เป็นอันดับหนึ่งแล้วกันครับ
P: 1- ตาม AAN guidelines เท่าที่รู้มาหากพบ ring-enhancing lesions ให้รักษาแบบ empirically for toxoplasmosis ไปก่อนครับwith: ceftriaxone และ vancomycin และdexamethasoneและphenytoin เพื่อป้องกันpyogenic brain abscess และยังปเองกัน seizure
2- ผมคิดว่าน่าจะ Biopsy เพื่อระบุเชื้อที่ถูกต้องและปรับยามาเชื้อต่อไป
3-ถ้าเป็น Norcardia : จะเป็นเป็น polymorphonucleated cells with gram-positive, modified acid-fast positive rods. ควรให้ยาtrimethoprim-sulfamethoxazole เป็น first line สำหรับ Second-line agents อาจะเป็น imipenem-cilastatin, amikacin, minocycline, ceftriaxone, หรือ dapsone
4-ควรตรวจ HIV ครับ อาจจะพบ
Posted by : KENNY , E-mail : (streptokinase@hotmail.com) ,
Date : 2010-09-12 , Time : 06:17:56 , From IP : 119.42.85.28
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}