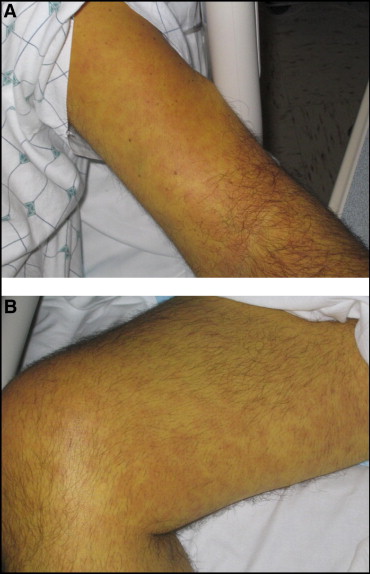
A 48-YOM presented with confusion, myalgias, and fever.ชายอายุ 48 ปีมีเพื่อนนำส่งรพ.เนื่องจากมีไข้ สับสนและปวดกล้ามเนื้อทั้งตัว. เขารู้ตัวดีแต่พูดไม่เป็นเรื่อง ตาเหลืองและตัวเหลือง เพื่อนเขาเล่าว่าผู้ป่วยไม่ค่อยอยู่บ้าน. -Examination of the patient revealed a temperature of 39.0° C, blood pressure of 70/50 mm Hg, heart rate of 96 beats per minute, and oxygen saturation of 96% on O2 (2 L/min). Asterixis and spider angiomata were present. His abdomen was soft with no hepatomegaly, but the splenic tip was palpable. -Laboratory studies were notable for a white blood cell (WBC) count of 55,000/mm3 with 21% immature forms; a hematocrit of 31.1%; and a platelet count of 31,000/mm3. Serum chemistry levels were: creatinine, 6.6 mg/dL; blood urea nitrogen, 173 mg/dL; total bilirubin, 51.6 mg/dL; direct bilirubin, 28 mg/dL; aspartate aminotransferase, 213 U/L; alanine aminotransferase, 146 U/L; alkaline phosphatase, 164 U/L; ammonia, 52 μmol/L; international normalized ratio, 1.1; lactate dehydrogenase, 568 U/L; Hepatitis C antibody was positive, but hepatitis B surface antigen and hepatitis A total antibody were negative. Human immunodeficiency virus-1 antibody was negative. 1. ผู้ป่วยมีปัญหาอะไรบ้างและการวินิจฉัยที่น่าจะเป็นที่สุดคืออะไร 2. จะ manage อย่างไร Posted by : cpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2010-09-06 , Time : 12:24:35 , From IP : 172.29.3.68 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}