ขอลองตอบครับ
-->ข้อ1.Unilateral rhinorrhea ในผู้ป่วยรายนี้น่าจะออกมาจากที่ไหน และจะตรวจยืนยันได้อย่างไร?
>สำหรับปัญหาเรื่อง unilateral rhinorrhea มี differential diagnosis ได้แก่ choanal atresia, nasal foreign body, nasal neoplasm, cerebrospinal rhinorrhea ทั้งนี้สองประการแรกนั้นมักตรวจพบในผู้ป่วยเด็กมากกว่า สำหรับสองประการหลังนี้อาจแยกเพียงตรวจโพรงจมูกดู อย่างไรก็ตามน้ำดังกล่าวไหลออกทางจมูกทุกครั้งเมื่อจามหรือไอ(เกี่ยวข้องกับการเพิ่ม ICP) หรือเวลาโน้มตัวไปข้างหน้า ทำให้นึกถึง CSF rhinorrhea ซึ่งเข้ากับประวัติดังกล่าวได้มากที่สุด หากนำรอยเปื้อนที่หมอนมาดู อาจจะพบ halo sign (รอยเลือดตรงกลางวงล้อมรอบด้วยรอยน้ำใส)
>สำหรับการตรวจยืนยันนั้น เนื่องจากสารคัดหลั่งอาจปนกับเลือดดังนั้นการส่ง Beta-2 transferrin ซึ่งเป็น carbohydrate-free isoform ของ transferring ซึ่งมีความจำเพาะหรือพบได้ใน CSF(sensitiviry ใกล้เคียง 100% และ specificity 95% โดย Beta-2 transferrin นี้พบได้เพียงใน perilymph, vitreous humor และ CSF เท่านั้น) โดยเลือดหรือ nasal secretion ไม่สามารถรบกวนผลตรวจได้
>สำหรับสาเหตุนั้น แม้ว่า traumatic leaks เป็นสาเหตุส่วนใหญ่กว่า 80% แต่ไม่มีประวัติอุบัติเหตุหรือผ่าตัด ดังนั้นอาจต้องคิดถึงกลุ่ม nontraumatic ได้แก่ brain tumors(intracranial และ extracranial tumor, cholesteatoma หรือ tuberculoma ซึ่งจะ erode กระดูกโดยตรง), skull base congenital defect และ meningoceles/meningoencephaloceles ในรายนี้คงต้องคิดถึง brain tumor เนื่องจากสาเหตุสองประการหลังมักตรวจพบในผู้ป่วยเด็ก
-->ข้อ2. จะ manage อย่างไร?
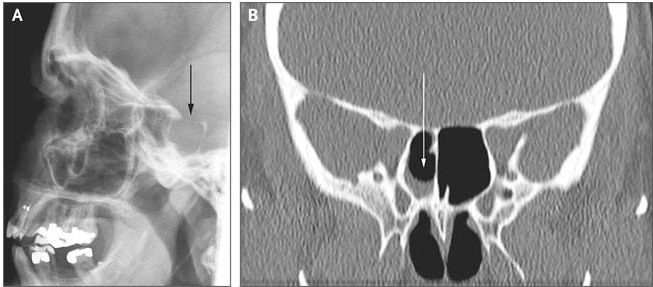
1.หลักการที่สำคัญของการรักษา CSF leakage คือ localization ของ dural defect โดยใช้ imaging ได้ CT/MRI
2.ให้ผู้ป่วยนอนบนเตียงยกหัวสูง, เลี่ยงการสูด/จาม/ไอ แรงๆ, ใช้ stool softeners
3.รอผล imaging เพื่อยืนยันการวินิจฉัยและดำเนินตามแนวทางการรักษาที่เหมาะสม
[ref: Abuabara A, Med Oral Patol Oral Cir Bucal. 2007 Sep 1;12(5):E397-400. Review.
Kerr JT, Otolaryngol Clin North Am. 2005 Aug;38(4):597-611. Review.]
Posted by : weeratian , Date : 2010-03-28 , Time : 20:07:02 , From IP : 112.142.28.229
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}