ความคิดเห็นทั้งหมด : 7
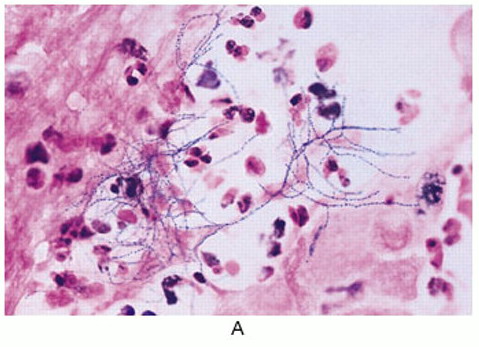
A 20-YOM had fevers with chills, productive cough, and weight loss for 1 month ชายอายุ 20 ปี เดิมแข็งแรงดี -7 เดือนก่อน ผู้ป่วยมีไข้อยู่นาน 3 สัปดาห์จึงไปรพ. การตรวจร่างกาย ตรวจทางห้องปฏิบัติการและภาพรังสีทรวงอกปกติ ต่อมาไข้ลงเอง และผู้ป่วยสบายดี -1 เดือนก่อน ผู้ป่วยเริ่มมีไข้หนาวสั่น ไอมีเสมหะและน้ำหนักลด ผู้ป่วยได้รับการรักษาที่รพ.แห่งหนึ่งซึ่งแพทย์ให้การวินิจฉัย community-acquired pneumonia และให้การรักษาด้วย ceftriaxone และ azithromycin ต่อมาแพทย์เพิ่มยา clindamycin แต่อาการยังคงเดิม เนื่องจากผู้ป่วยยังมีไข้และไอจึงย้ายผป.มาที่รพ.ใหม่ ผู้ป่วยไม่เคยป่วยเป็นโรคใดๆ ไม่มีประวัติสัมผัสผู้ป่วยโรคใดๆหรือสัตว์ และการเดินทาง ผู้ป่วยเป็นนักศึกษา ไม่สูบบุหรี่ ไม่ดื่มและไม่ติดยาใดๆ At admission to new hospital, the patient was febrile and dyspneic, with bilateral fine crackles heard on lung examination. CBC: hemoglobin level, 11 g/dL, WBC, 21,000 cells/μL with a left shift and platelet count, 420,000 platelets/μL). erythrocyte sedimentation rate was 92. ในรูป A คือภาพรังสีทรวงอก 1. ผู้ป่วยน่าจะเป็นโรคใด 2. จะ manage อย่างไรต่อไป Posted by : cpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2010-03-16 , Time : 15:58:13 , From IP : 172.29.3.68 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}