ขอลองตอบครับ
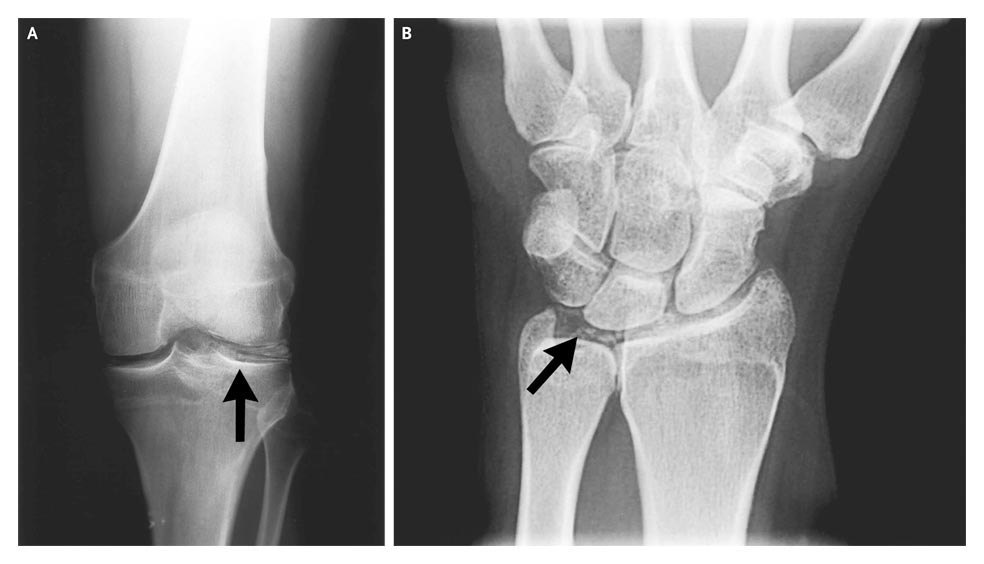
-->ข้อ1.ในรูป A และ B คือภาพรังสีของเข่าและข้อมือ พบความผิดปกติอะไรบ้าง?
ภาพที่เห็นเป็น calcification เป็นเส้น โดยตำแหน่งเป็น cartilage ของเข่าด้านซ้าย โดยลูกศรชี้ตำแหน่ง lateral meniscus ส่วน film PA hand ด้านซ้าย ก็เห็นเป็น chondrocalcinosis ไม่มี scapholunate widening ไม่มี disruption ของ sacpholunate ligament [ซึ่งลักษณะนี้พบได้ในหลายโรค ได้แก่ DJD, CPPD, Gout, Acromegaly, Hemochromatosis, Hyperparathyroidism, Ochronosis, Wilson’s disease, Oxalosis] นอกจากนี้ไม่พบ cystic changes, erosion with sclerotic margin with overhanging bony edges ซึ่งบ่งชี้นำให้คิดถึง gout
-->ข้อ2. การวินิจฉัยคืออะไร
จากประวัติการปวดข้อเป็น polyarthritis (?symmetry) ซึ่งเป็น chronic pain แต่มีอาการ acute attack เป็นครั้งคราว ประวัตินี้ทำให้คิดถึงกลุ่ม crystal-induced ได้แก่ gout ซึ่งมักเกิดในเพศชายวัยกลางคนหรือสูงอายุ หรือในผู้หญิงวัยหลังหมดประจำเดือน หรือ pseudogout ซึ่งก็มักเกิดวัยสูงอายุ แต่ข้อค้านของ gout ได้แต่ 1.ตำแหน่งของพยาธิสภาพไม่ใช่ common site 2.ช่วงแรกของอาการอยากเห็นลักษณะ mono หรือ oligoarticular มากกว่า polyarticular (สำหรับ CPPD เป็น polyarticular lesion มากกว่า 2/3 ของผู้ป่วย) ดังนั้นในผู้ป่วยรายนี้คงคิดถึง CPPD มากกว่าเนื่องจาก joint distribution เป็น clue ที่สำคัญโดยบริเวณเข่าเป็นตำแหน่งที่พบบ่อยที่สุด (นอกจากนี้ได้แก่ wrist, shoulder, ankle, elbow และ hands) และภาพรังสีก็เข้าได้กับ CPPD นอกจากนี้อาจคล้ายคลึงกับ slowly progressive osteoarthritis แต่หากเป็น primary OA นั้นพยาธิภาพบริเวณข้อมือพบได้น้อยมาก
สำหรับ hypomagnesaemia นั้นก็สัมพันธ์กับ CPPD อย่างมาก โดยมีสาเหตุได้หลายประการได้แก่ Gitelman syndrome, short bowel syndrome และ familial renal magnesium wasting โดยสาเหตุดังกล่าวนั้นเป็นสาเหตุของ chondrocalcinosis และ CPPD arthropathy นอกจากนี้พบว่ายา thiazide diuretics สามารถทำให้เกิด chondrocalcinosis ได้ ดังนั้นจึงมีข้อแนะนำให้ส่ง magnesium level ในผู้ป่วย CPPD ทุกกลุ่มอายุ โดยเฉพาะผู้ป่วยที่ได้รับ thiazide
-->ข้อ3. จะ manage อย่างไร?
1.สำหรับ definitive diagnosis คงต้องส่ง synovial fluid โดยจะพบ WBC หลายพันถึง 100,00 cells/uL รวมถึงมี neutrophil เด่น และ Polarized light microscopy พบ rhomboid, square, หรือ rod-like crystals with weak positive birefringence ภายใน tissue fragments/fibrin clots และใน neutrophils
2.การรักษานั้นหากมี joint effusion นั้น joint aspiration อาจสามารถลดอาการได้ นอกจากนี้อาจให้ NSAIDs หรือ intra-articular glucocorticoid injection และหากมี recurrent attacks คงต้องให้ daily prophylactic treatment คือ low dose ของ colchicines อาจมีประโยชน์
3.สำหรับ hypomagnesemia คงรักษาโดยให้ oral Mg salts (500-1000 mg PO tid for 3-4 days) และนัดติดตามค่า Mg จนมีอยู่ในค่าปกติและนัดติดตามประเมินอาการปวดของผู้ป่วย
[ref: Harrison Internal Medicine 17ed: Chapter 327-Gout and Other Crystal Arthropathies]
Posted by : weeratian , Date : 2010-02-09 , Time : 00:06:59 , From IP : 172.29.22.75
|
{kind=link}
{kind=link}
{kind=link}