ความคิดเห็นทั้งหมด : 2
A 28-YOW with SLE had abdominal pain with nausea and vomiting for 2 days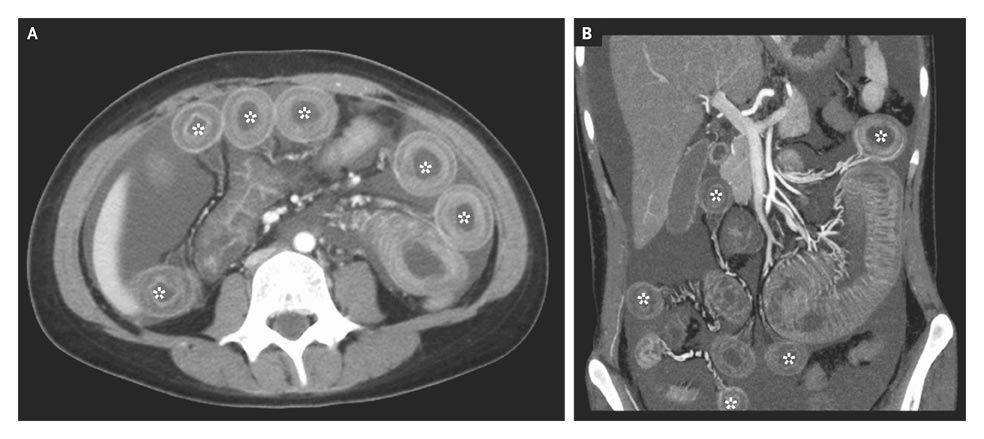 หญิงอายุ 28 ปีเข้ารับการรักษาในรพ.เนื่องจากปวดท้องรอบสะดือหลังกินอาหารและมีคลื่นไส้อาเจียนมานาน 2 วัน ผู้ป่วยกินยา prednisolone 10 มก/วันอยู่ประจำ เมื่อ 3 ปีก่อน เธอได้รับการวินิจฉัย SLE เพราะมี malar rash, proteinuria, high-titer antinuclear antibodies และ elevated anti–double-stranded DNA antibodies. On admission, she was afebrile and normotensive, and the physical examination revealed only diffuse abdominal distention and mild rebound pain without rigidity; occult testing of stool for the presence of blood was negative. A laboratory evaluation was unremarkable except for a platelet count of 90,000 per cubic millimeter, hypocomplementemia, and elevated levels of anti–double-stranded DNA antibodies. Antiphospholipid antibodies were not detected. 1. ในรูป A และ B คือ computed tomography of the abdomen พบความผิดปกติอะไรบ้าง (ความสำคัญอยู่ที่ *) 2. อาการปวดท้องของผู้ป่วยน่าจะเกิดจากอะไรมากที่สุด 3. จะ manage อย่างไร Posted by : chpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2010-01-04 , Time : 08:11:37 , From IP : 172.29.3.68 |

{kind=link}
{kind=link}
{kind=link}