ขอลองตอบครับ
-->ข้อ1. ปัญหาของผู้ป่วยคืออะไร
1.acute undifferentiated fever with diarrhea with splenomegaly with Hemolytic anemia
2.History of returning from travel abroad
3.Increased creatinine level-acute renal failure
-->ข้อ2. การวินิจฉัยที่น่าจะเป็นคือ..............
: ) สำหรับ acute undifferentiated fever นั้น ได้แก่ 1.viral(influenza, dengue) 2.Rickettsia 3.Leptospirosis 4.Malaria 5.Typhoid fever 6.Bacteremia การท่องเที่ยวกลับมาจากบริเวณหนึ่งสัมพันธ์กับปัจจัยเสี่ยงของ specific disease ยกตัวอย่างเช่น malaria เป็นสาเหตุของไข้เมื่อผู้ป่วยเดินทางกลับมาจาก Sub-Saharan Africa หรือ Oceania ตรงนี้จะแสดงถึงความสำคัญของระบาดวิทยาที่ช่วยในการวินิจฉัยโรค อีกทั้งการถามวันที่กลับมาจากแหล่งท่องเที่ยวและ onset ของอาการจะช่วยวินิจฉัยโรคได้จากการพิจาราณา incubation period (โรคที่อาจเป็นไปได้ ได้แก่ 1.malaria[7-70days] 2.typhoid fever[5-21days, มี diarrheal illness เมื่อ 2 สัปดาห์]) ทั้ง malaria และ typhoid fever สามารถทำให้เกิดอาการ fever, headache, abdominal pain และ gastrointestinal symptoms ได้เช่นกัน (แม้ว่า Salmonella จะทำให้เกิด infection ที่ Peyer patches แต่ typhoid fever ทำให้เกิด constipation มากกว่า diarrhea) สำหรับอาการปวดท้องในผู้ป่วยรายนี้ ซึ่งหากตรวจร่างกายหรือinvestigation เช่น ultrasound สนับสนุน intra-abdominal bleeding สิ่งที่น่ากังวลที่สุดคือภาวะ splenic rupture
: ) สำหรับผู้ป่วยรายนี้คิดถึง Malaria มากที่สุด เพราะ 1].ข้อมูลระบาดวิทยานั้น malaria มี prevalence ใน South Asia และ Sub-Saharan Africa มาก(เกาะ Madagascar เป็นเกาะที่อยู่ใน Indian ocean ทางตะวันออกเฉียงใต้ของ Africa) 2].มีอาการที่เข้าได้ (โดยอาการที่พบได้คือ fever 100%, headache 100%, weakness 94%, profuse night sweats 91%, insomnia, 69%, arthralgias 59%, myalgias 56%, diarrhea, 13%, abdominal cramps 8% 3].ตรวจร่างกายก็จะพบ pallor และ hepatosplenomegaly 4].malaria สามารถอธิบาย hemolytic anemia ในผู้ป่วยรายนี้ได้(Hb ต่ำ, LDH และ bilirubin สูง) ส่วนค่า creatinine ที่สูงขึ้นก็สามารถอธิบายได้จาก malaria ซึ่งประกอบด้วยหลายปัจจัยคือ dehydration, increased metabolism และ impaired renal function
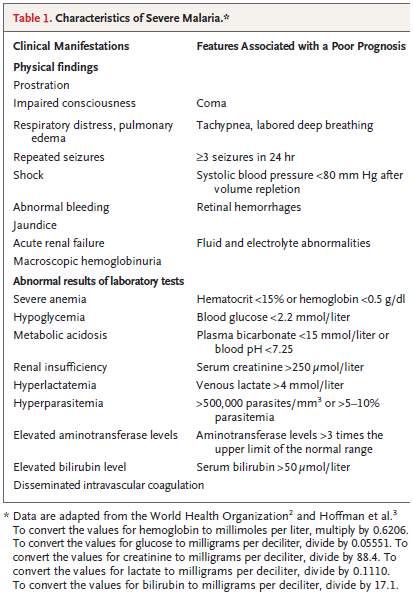
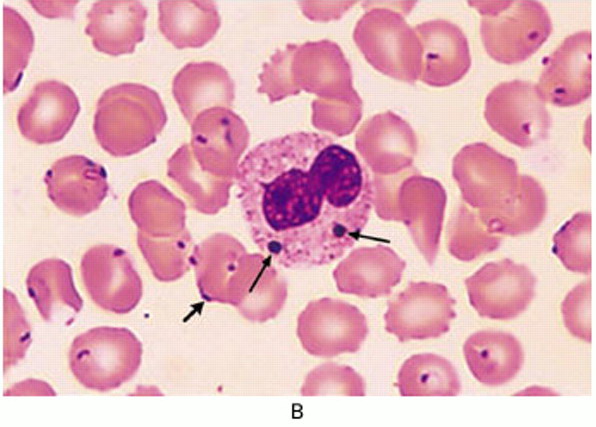
: ) ขอตอบว่าการวินิจฉัยผู้ป่วยรายนี้เบื้องต้นคิดถึง malaria (ซึ่งมีความรุนแรง-severe เนื่องจากมี bilirubine สูงมาก, acute renal failure)
-->ข้อ3. จะส่ง investigate อะไร
1.Light microscopy of Giemsa-stained blood smears: Thick และ thin smear 2.Blood culture (for Salmonella detection) 3.Electrolyte 4.ทำ US-abdomen
Ref:
1.Emerg Med Clin North Am. 2008 May;26(2):499-516, x.
2.DAVID O. FREEDMAN, Ch 329 Infections in Returning Travelers, Mandell, Bennett, & Dolin: Principles and Practice of Infectious Diseases, 6th ed.
3.Artesunate for the treatment of severe falciparum malaria. N Engl J Med. 2008 Apr 24;358(17):1829-36.
Posted by : weeratian , Date : 2009-08-22 , Time : 12:21:52 , From IP : 172.29.11.244
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}