ความคิดเห็นทั้งหมด : 5
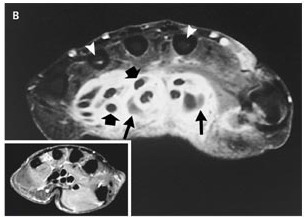
A 60-year-old woman presented with a painful left hand หญิงอายุ 60 ปี มาตรวจเนื่องจากเจ็บมือซ้ายมา 1 เดือน เมื่อ 3 เดือนก่อน ผู้ป่วยถูกเสี้ยนไม้ตำที่นิ้วหัวแม่มือซ้ายและได้ดึงเสี้ยนออกเองออก ผู้ป่วยได้รับการรักษาด้วยยาปฏิชีวนะและ NSAID แต่อาการกลับเป็นมากขึ้น รอยโรคจากเดิมที่มีการอักเสบและกดเจ็บเฉพาะที่นิ้วหัวแม่มือ กลายเป็นลุกลามเป็นบวมทั้งมือ ข้อมือและแขนซ้ายร่วมกับกดเจ็บและขยับไม่ได้ On examination, the patient appeared healthy and had a temperature of 37.1°C. Her left hand was diffusely swollen, and her fingers were in a semiflexed position. The center of her palm was warm and puffy, and her volar forearm proximal to her left wrist had a red, raised, inflamed area that measured 7 by 5 cm (รูป A, arrow). There was no palpable epitrochlear or axillary adenopathy. Her white-cell count was 8700/cumm. 1. การวินิจฉัยที่น่าจะเป็นคือ.................................................. 2. จะ manage อย่างไรต่อ Posted by : chpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2009-07-29 , Time : 15:40:57 , From IP : 172.29.3.68 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}