ความคิดเห็นทั้งหมด : 3
A 53-YOM had abnormal of his eyes and pain &numbness of left arm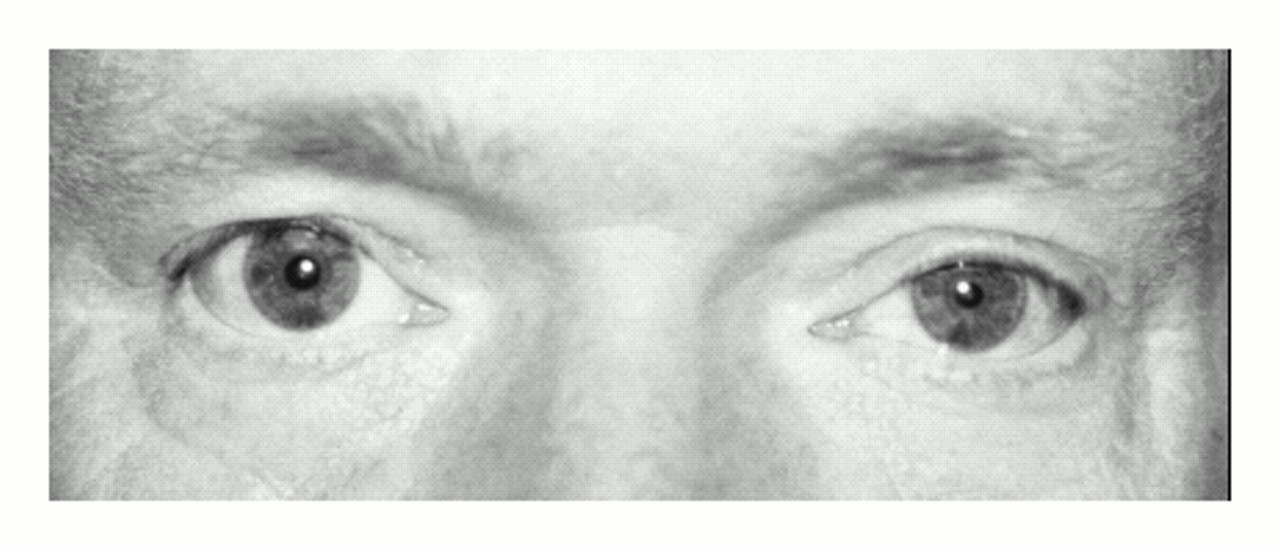 ชายอายุ 53 ปีถูกส่งตัวมาปรึกษาเนื่องจากมีความผิดปกติของตาซ้ายดังในรูป A เขาปวดและชาที่แขนซ้ายร่วมกับเหงื่อออกน้อยลงที่หน้าด้านซ้ายมานาน 9 เดือน 1. ความผิดปกติของตาคือ.................................................. 2. กลุ่มอาการนี้คือ.............................................................. 3. จะ manage อย่างไรต่อไป Posted by : chpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2009-07-03 , Time : 09:52:15 , From IP : 172.29.3.68 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}