ความคิดเห็นทั้งหมด : 2
A 15-YOB had tachypnea & became coma 2 hours after onset of fever & malaise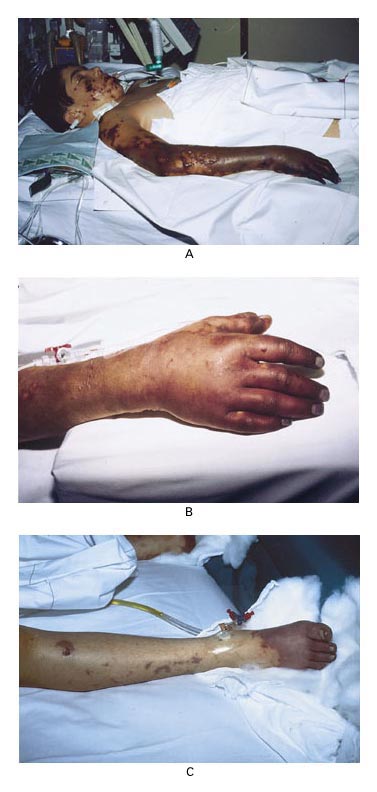 เด็กชายอายุ 15 ปี ถูกนำส่งห้องฉุกเฉินเนื่องจากมีใจเต้นเร็ว หอบและหมดสติซึ่งเกิดขึ้น 2 ชั่วโมงหลังจากที่เขาเริ่มมีไข้และอ่อนเพลีย ที่ห้องฉุกเฉิน pulse 180/min; blood pressure 70/45 mm Hg; temperature 40.2°C; His hands and feet were cool and cyanotic. He had no signs of meningeal irritation. 1. ผู้ป่วยมีรอยโรคที่ผิวหนังดังในรูป พบความผิดปกติอะไรบ้าง 2. การวินิจฉัยคือ.................................................. 3. จะ manage อย่างไร Posted by : chpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2009-06-23 , Time : 15:41:08 , From IP : 172.29.3.68 |
{kind=link}
{kind=link}
{kind=link}