ขอบคุณคุณหมอ aomnaka มากค่ะ คุณหมอตอบถูกต้องแล้วนะคะ
การรักษา neurosyphilis ที่ highly recommend คือ Aqueous crystalline penicillin G 18-24 mU/day, administered as 3-4 mU IV every 4 hours or continuous infusion, for 10--14 days.
ผู้ป่วยรายนี้ได้รับ penicillin therapy นาน 10 วันแล้วผู้ป่วยไม่ยอมรับยาต่ออีก หลังจากนั้นผู้ป่วยไม่ได้ไปพบแพทย์อีกเลย จนกระทั่ง 12 เดือนต่อมา
ผู้ป่วยได้มาตรวจอีกเนื่องจากอาการความจำเสื่อม เดินและพูดลำบาก
PE: the patient was disoriented with episodes of aggressiveness. His mini mental state examination (MMSE) score was 9/30. The rest of the neurological examination was normal.
Results of standard laboratory tests and concentrations of thyroid hormones, vitamin B12, and folic acid were normal.
-HIV and hepatitis B and C serology was negative.
-Protein 14-3-3, s-100, and TauAg in CSF were normal.
-CSF sample showed a normal cell count and protein concentration, with positive oligoclonal IgG bands indicating intrathecal synthesis.
Syphilis serology in serum and CSF was positive.
serum -Venereal Disease Research Laboratory test [VDRL] was 1:32,
-TPHA 1:5120
-IgG fluorescent treponemal antibody absorption test [IgG-FTA-ABS] 1:320;
CSF - TPHA was 1:160,
- IgG-FTA-ABS 1:4
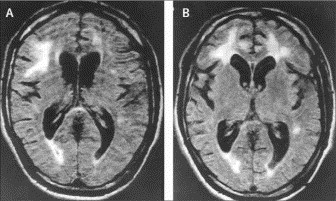
Brain MRI : numerous white-matter hyperintensities which did not show post-contrast enhancement.
MRI of the cervical spinal cord was normal.
ผู้ป่วยได้รับ aqueous crystalline penicillin G 24 mU/day (4 mU IV ทุก 4 ชม.) นาน 4 สัปดาห์ จากการติดตามผู้ป่วยนาน 6 เดือน เขาไม่มีอาการผิดปกติใหม่ๆ ทางระบบประสาท และมี MMSE score 11/30
ในปัจจุบัน อุบัติการณ์ของ syphilis เพิ่มขึ้นทั่วโลก ซึ่งสามารถอธิบายได้บางส่วนจากการเพิ่มของการติดเชื้อ HIV infection พฤติกรรมทางเพศ การเดินทางและการอพยพ และปัจจัยทางการเมือง เศรษฐกิจ และสังคม ผู้ป่วยรายนี้เป็น neurosyphilis โดยที่เขาเป็น immunocompetent ทราบกันดีว่าsyphilis เป็น the great mimicker และ neurosyphilis ก็เช่นเดียวกัน neurosyphilis สามารถทำให้เกิดความผิดปกติทาง neuroimaging ได้เหมือนกับที่พบใน herpes simplex encephalitis, mesial temporal sclerosis, leucoaraiosis, normal-pressure hydrocephalus และ glioblastoma multiforme ผู้ป่วยที่มีneurosyphilis สามารถมี MRI brain ที่ปกติ หรือมีเพียง temporal-lobe atrophy CSF finding เป็นได้ตั้งแต่ positive oligoclonal IgG bands และ IgG index สูง จนถึง pleocytosis โดยอาจมีหรือไม่มี positive CSF VDRL ดังนั้น การให้การวินิจฉัย neurosyphilis จึงยังคงมีปัญหาอยู่แม้ว่าในปัจจุบันจะมีการความก้าวหน้าด้านการตรวจต่างๆ
แพทย์ต้องนึกถึงไว้เสมอว่า dementia ในผู้ป่วยอายุน้อยที่มี temporal-lobe atrophy และ/หรือ demyelination สามารถเกิดขึ้นได้จาก syphilis จึงจำเป็นต้องตรวจ CSF และ syphilis testing
Posted by : chpantip , E-mail : (chpantip@medicine.psu.ac.th) ,
Date : 2008-09-23 , Time : 15:39:19 , From IP : 172.29.3.68
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}