ความคิดเห็นทั้งหมด : 3
หญิง 61 ปี มีไข้ต่ำๆ มีก้อนที่ด้านหน้าของคอ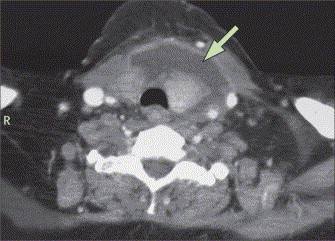 หญิงอายุ 61 ปี มาที่ ER ด้วยเรื่องเจ็บคอ ไข้ต่ำๆ มีก้อนกดเจ็บที่ด้านหน้าของคอและเจ็บที่ก้อนมากขึ้นเวลากลืนมานาน 1 สัปดาห์ ผู้ป่วยกินยา cephalexin มา 5 วัน PE: afebrile, alert, พูดคล่องแต่เสียงแหบ, tachycardic had a soft, mobile, and tender erythematous anterior cervical swelling. Flexible nasopharyngoscopy: diffuse supraglottic edema and erythema with a thick purulent fluid lacing the piriform sinuses. White blood count was 25,600/cumm with 81% neutrophils. 1. ในรูปคือ CT of the neck พบความผิดปกติอะไรบ้าง 2. การวินิจฉัยโรคคืออะไร 3. จะ manage อย่างไรต่อไป Posted by : chpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2008-09-17 , Time : 14:33:02 , From IP : 172.29.3.68 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}