{kind=link}
{kind=link}
{kind=link}
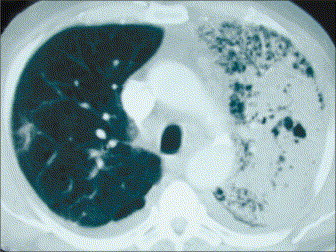 ขอบคุณคุณหมอ sagittareusinternist และนศพ.harder มากค่ะ ยินดีต้อนรับสู่ e-consult ค่ะ แพทย์ได้เจาะและระบายหนองฝีที่จมูกพร้อมให้ยา amoxicillin/clavulanic acid, and amikacin ผลการเพาะเชื้อจากเลือดและหนองจากจมูกขึ้น methicillin-susceptible Staphylococcus aureus ในช่วงสัปดาห์แรกของการรักษา ผู้ป่วยหอบเหนื่อยมากขึ้น ได้ทำ Chest CT วันที่ 6 ของการรักษา ถาม 1. พบความผิดปกติอะไรจาก Chest CT บ้าง 2. ท่านจะส่ง work up อะไรบ้างเพื่อให้ทราบถึง virulence factor ของเชื้อนี้ Posted by : chpantip , E-mail : (chpantip@medicine.psu.ac.th) , Date : 2008-09-10 , Time : 15:35:46 , From IP : 172.29.3.68 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}